

Incidental Pulmonary Nodules: Differentials and Diagnostic Imaging
Incidental findings (or “incidentalomas”) are a reality of modern medicine. As CT imaging becomes increasingly common, clinicians are more frequently faced with unexpected results that require thoughtful interpretation and follow-up. One of the most common (and anxiety-provoking) are incidental pulmonary nodules (IPNs).
As primary care providers, we are often responsible for managing these findings long after the emergency department visit or imaging indication has passed. Knowing how to approach IPNs systematically can reduce unnecessary testing, avoid missed diagnoses, and help reassure patients.
A Common Clinical Scenario
A 50-year-old male presents for follow-up after an emergency department visit. A CT chest was performed to rule out pulmonary embolism, which was negative. However, the report notes an incidental pulmonary nodule, and follow-up is recommended.
The patient looks to you for answers.
What does this mean?
How worried should they be?
What happens next?
What Is an Incidental Pulmonary Nodule?
A pulmonary nodule is a focal area of increased attenuation (i.e. appears whiter, brighter) in the lung that measures less than 30 mm (3 cm) in diameter.
Micronodule: < 6 mm
Pulmonary nodule: < 30 mm
Pulmonary mass: > 30 mm
An incidental pulmonary nodule is one that is discovered unintentionally on imaging performed for an unrelated reason, such as:
CT chest for pulmonary embolism
Trauma CT
Cardiac CT
Abdominal CT
Occasionally chest X-ray (*usually larger nodules show up on these)
The increased use of CT imaging has led to a parallel rise in incidental findings (IPNs included).
How Common Are IPNs?
Pulmonary nodules are detected in approximately 20–30% of CT chest scans.
The good news: Most nodules are benign, commonly representing:
Granulomas
Hamartomas
Sequelae of prior infection
However, 5–7% of nodules may represent early lung cancer, particularly in higher-risk populations, which is why appropriate evaluation matters.
Why IPNs Matter in Primary Care
Primary care clinicians play a central role in IPN management:
Interpreting radiology reports
Communicating risk clearly to patients
Ensuring appropriate follow-up imaging
Coordinating care with radiology and specialists
Despite clear guidelines, studies suggest that up to two-thirds of Canadian patients do not receive recommended follow-up for incidental pulmonary nodules. This creates both patient safety risks and medico-legal vulnerability.
A Nodule Is Identified — What’s the Differential?
The differential diagnosis for a pulmonary nodule is broad, ranging from benign to malignant causes.
Benign Differentials
| Category | Differential Diagnosis |
|---|---|
| Infectious |
Granulomas (sequelae from infection) Mucous plug Abscess Septic embolism Round pneumonia |
| Non-infectious |
AV malformation Lymph node Rheumatoid nodule Amyloidoma Scarring Granulomatosis with polyangiitis |
| Congenital |
Pulmonary sequestration Bronchial atresia Bronchogenic cyst |
Malignant Differentials
| Category | Differential Diagnosis |
|---|---|
| Primary lung cancer |
Non-small cell lung cancer (most common — adenocarcinoma, squamous cell carcinoma, large cell carcinoma) Small cell lung cancer |
| Metastasis | Cancer has travelled from a primary tumor elsewhere in the body to the lungs, often appearing as multiple nodules |
*Importantly, less than 10% of IPNs are malignant. Risk assessment depends on both patient factors and nodule characteristics.
Risk Factors for Malignancy
| Risk Category | Risk Factors |
|---|---|
| Patient-related risk factors |
Smoking history (current or former; especially >30 pack-years) Emphysema on CT (independent risk factor) Age >50 years (lung cancer is rare under 35) Family history (especially a sibling) Pulmonary fibrosis (particularly idiopathic pulmonary fibrosis) *Smoking increases lung cancer risk by 10–35 fold. |
| Environmental risk factors |
Asbestos Uranium Radon |
| Nodule-related risk factors |
Size: Larger nodules carry higher risk Estimated malignancy risk by size: <3 mm: ~0.2% 4–6 mm: ~0.9% 6–8 mm: 1–5% 8–12 mm: 10–20% 20 mm: ~50% Margins: Spiculated or lobulated margins are more concerning Location: Upper-lobe nodules are higher risk Growth over time: Growth increases suspicion Number: 1–4 nodules are more concerning than >5 |
How Radiologists Report IPNs
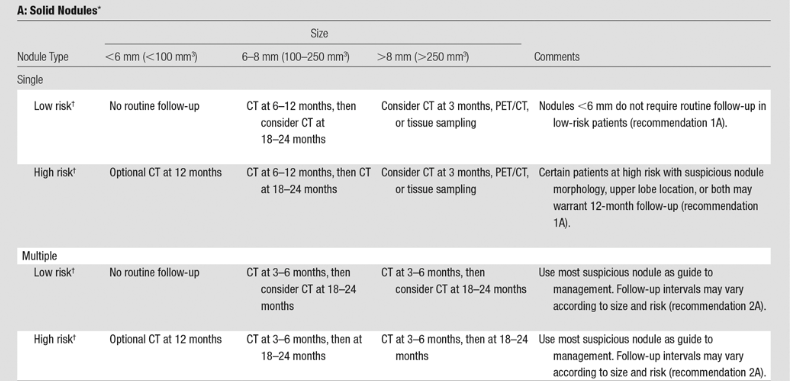
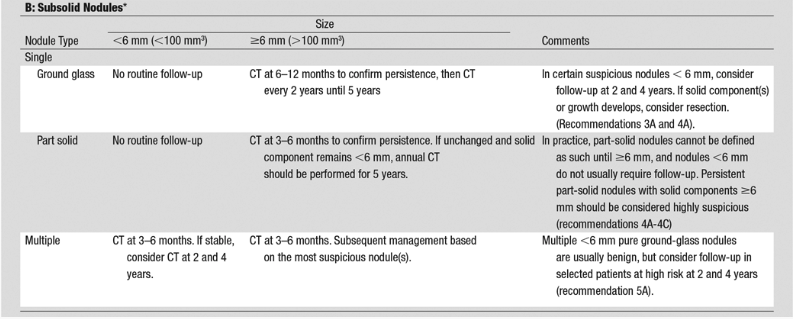
Most radiology reports follow Fleischner Society (2017) recommendations, which guide follow-up for incidental nodules detected on CT.
Key imaging features reported include:
| Imaging Feature | Interpretation & Clinical Significance |
|---|---|
| 1. Nodule size (mean diameter) |
Small: <6 mm Intermediate: 6–8 mm Large: >8 mm |
| 2. Attenuation |
Calcified nodules: Often suggest benign disease Solid nodules: Completely obscure underlying lung architecture Subsolid nodules: – Ground-glass nodules – Part-solid nodules (ground-glass + solid component) |
| 3. Number and location |
Single vs multiple nodules Upper-lobe nodules (especially right upper lobe) are higher risk Juxtapleural or perifissural nodules are often benign Adjacent cystic airspaces increase malignancy risk |
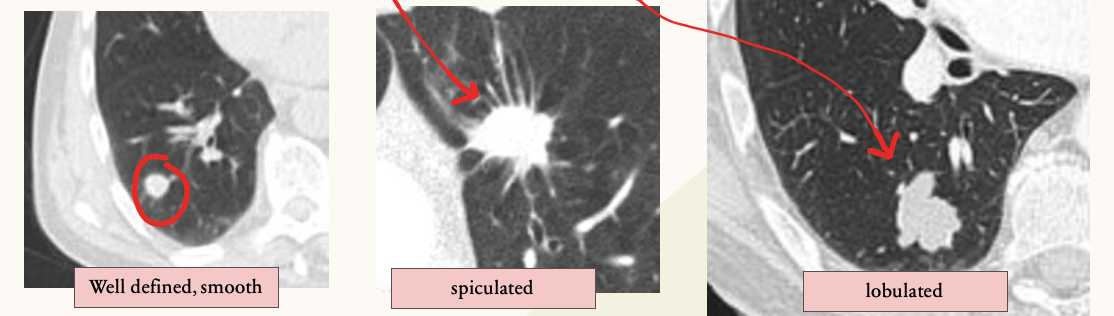
| 4. Margins |
Smooth, well-defined margins are less suspicious Ill-defined, spiculated, or lobulated margins raise concern |
| 5. Growth and doubling time |
Solid nodules: Stable for 2 years → benign Subsolid nodules: Require up to 5 years of stability Growth over time increases suspicion for malignancy |
Source: Snoeckx A, Reyntiens P, Desbuquoit D, Spinhoven MJ, Van Schil PE, van Meerbeeck JP, Parizel PM (February 2018). "Evaluation of the solitary pulmonary nodule: size matters, but do not ignore the power of morphology". Insights into Imaging. 9 (1): 73-86. doi:10.1007/s13244-017-0581-2.
Initial Management of an Incidental Pulmonary Nodule
Before applying guideline recommendations, confirm that this truly qualifies as an incidental pulmonary nodule.
Fleischner guidelines apply only if:
Age >35 years
Incidental finding
No known active cancer
Not immunocompromised
No clinical suspicion of infection
Not part of a lung cancer screening program
Plain (non-contrast) CT is sufficient for follow-up in most cases.
Back to the Case: review risk factors for our patient
Age: 50
Not immunocompromised
No smoking history
No family history of lung cancer
No emphysema or known exposures
CT report: Incidental 6 mm solid pulmonary nodule in the left lower lobe. Recommendation: follow-up CT in 6–12 months.
This recommendation aligns with guideline-based management for a low-risk patient with a small solid nodule.
Risk-Stratified Follow-Up
Management depends on:
Patient risk factors
Nodule size and features
Whether the nodule is solid or subsolid
Single vs multiple nodules
Transient nodules that resolve do not require follow-up. Persistent nodules require risk-based surveillance.
Always consider whether the patient should instead be followed through a lung cancer screening program, if eligible.
Communication Matters
Effective IPN management isn’t just about imaging, it’s about communication with our colleagues:
Provide radiology with relevant clinical history
Inform radiologists of prior imaging when available
AND clear communication with our patients:
Managing fear of cancer → Emphasize that nodules are common, not a cancer diagnosis
Confusion about follow-up → Explain risk using size, appearance, and patient factors. Observation is evidence-based and safer than unnecessary testing
Address radiation concerns
When to Refer
Referral to respirology or thoracic surgery should be considered for:
Growing nodules
Persistent nodules >8 mm
Nodules with suspicious imaging features
A Note on Incidental Nodules on Chest X-Ray
If an IPN is first detected on chest X-ray:
Small nodules without comparison → repeat X-ray in 6–8 weeks (?resolving infectious process)
Larger nodules or high-risk patients → CT chest
Key Takeaways
Incidental pulmonary nodules are common and usually benign
Risk stratification using patient and nodule factors is essential
Evidence-based guidelines help avoid over- or under-management
Thoughtful follow-up improves patient safety and reduces harm
ReferencesHansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008 Mar;246(3):697–722.MacMahon H, Naidich DP, Goo JM, Lee KS, Leung ANC, Mayo JR, et al. Guidelines for management of incidental pulmonary nodules detected on CT images: from the Fleischner Society 2017. Radiology. 2017 Jul;284(1):228–243.Callister MEJ, Baldwin DR, Akram AR, Barnard S, Cane P, Draffan J, et al. British Thoracic Society guidelines for the investigation and management of pulmonary nodules. Thorax. 2015 Aug;70(Suppl 2):ii1–ii54.Aberle DR, Adams AM, Berg CD, Black WC, Clapp JD, Fagerstrom RM, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011 Aug;365(5):395–409.Horeweg N, Scholten ET, de Jong PA, van der Aalst CM, Weenink C, Lammers JWJ, et al. Detection of lung cancer through low-dose CT screening (NELSON): a prespecified analysis of screening test performance and interval cancers. Lancet Oncol. 2014 Nov;15(12):1342–1350.Horeweg N. Lung cancer screening in the NELSON trial: balancing harms and benefits [dissertation]. Rotterdam (NL): Erasmus University Rotterdam; 2014.Gould MK, Tang T, Liu IL, Lee J, Zheng C, Danforth KN, et al. Recent trends in the identification of incidental pulmonary nodules. Am J Respir Crit Care Med. 2015 Nov;192(10):1208–1214.Hendrix W, Rutten M, Hendrix N, van Ginneken B, Schaefer-Prokop C, Scholten ET, et al. Trends in the incidence of pulmonary nodules in chest CT: 10-year results from two Dutch hospitals. Eur Radiol. 2023 Nov;33(11):8279–8288.Simon M, Zukotynski K, Naeger DM. Pulmonary nodules as incidental findings. CMAJ. 2018 Feb;190(6):E167.Snoeckx A, Reyntiens P, Desbuquoit D, et al. Evaluation of the solitary pulmonary nodule: size matters, but do not ignore the power of morphology. Insights Imaging. 2018 Feb;9(1):73–86.Ko JP, Azour L. Management of incidental lung nodules. Semin Ultrasound CT MR. 2018 Jun;39(3):249–259.Truong MT, Ko JP, Rossi SE, et al. Update in the evaluation of the solitary pulmonary nodule. Radiographics. 2014 Oct;34(6):1658–1679.Bartholmai BJ, Wan Koo C, Johnson G, et al. Nodule characterization, including computer analysis and quantitative features. J Thorac Imaging. 2015 Mar;30(2):139–156.Bankier AA, MacMahon H, Goo JM, Rubin GD, Schaefer-Prokop CM, Naidich DP. Recommendations for measuring pulmonary nodules at CT: a statement from the Fleischner Society. Radiology. 2017 Nov;285(2):584–600.Nair A, Bartlett E, Walsh S, et al. Variable radiological lung nodule evaluation leads to divergent management recommendations. Eur Respir J. 2018 Dec;52(6):1801359.Shen Y, Xu X, Zhang Y, et al. Lung cancers associated with cystic airspaces: CT features and pathologic correlation. Lung Cancer. 2019 Sep;135:110–115.Mets OM, Schaefer-Prokop CM, de Jong PA. Cyst-related primary lung malignancies: an important and relatively unknown imaging appearance of (early) lung cancer. Eur Respir Rev. 2018 Dec;27(150):180079.