

Neutropenia Differentials and Lab Test Interpretation
Mild neutropenia shows up unexpectedly — here’s a structured approach that saves time and anxiety.
🔎Case: You’re reviewing lab results for a 40-year-old patient. A CBC with differential reveals neutropenia; all other parameters are normal.
The CBC was ordered as part of a routine check-up, at the patient’s request, “just in case.”
There are no prior CBC results on file to compare trends in neutrophil counts or other indices.
The absolute neutrophil count (ANC) is:
1.2 × 10³/µL (1200 cells/µL)
The Cost of Routine Testing
Incidental findings are common in primary care, particularly when CBCs are ordered for routine screening without clear clinical indications.
While each result may seem minor, the cumulative burden is not.
On average, avoiding routine CBCs in patients without clear indications could save 1.5 hours per month per clinician. That translates to:
2 days per year
8 weeks over a 25-year career
In a 10-clinician practice: 20 clinic days freed annually
That’s time that could be redirected toward high-value care and patients who truly need attention (1).
I’ve certainly been guilty of this practice pattern in the past. Now, I use a cognitive forcing strategy before ordering any test:
What am I looking for?
How will a positive or negative result change management?
What differential am I trying to narrow?
What will I do if the result is abnormal?
Still: once an abnormality appears, we are responsible for addressing it.
💡Bottom line: Avoid annual screening blood tests unless directly indicated by the patient’s risk profile.
What is Neutropenia?
Neutropenia is a decrease in circulating neutrophils. In adults, it is typically defined as:
ANC < 1.5 × 10³/µL (<1500 cells/µL)
The absolute neutrophil count is reported as part of the WBC differential. Neutrophils are the most abundant white blood cells and serve as the first line of defense against infection - migrating to sites of inflammation, ingesting pathogens, and facilitating microbial destruction (2,3).
Classification of Neutropenia:
Mild: >1.0 – 1.5 x 10³/µL
Moderate: >0.5 - <1.0 x 10³/µL
Severe: <0.5 x 10³/µL
Agranulocytosis: <0.2 x 10³/µL
Chronic neutropenia: lasting for >3 months.
How common is neutropenia in adults?
Prevalence varies depending on the population studied. Normal reference ranges differ among ethnic groups, which affects reported rates (2).
Neutropenia is reported in <1% to 10% of healthy, asymptomatic individuals. Rates are higher in patients with certain medical conditions, such as autoimmune or connective tissue diseases (2).
💡Practice point: the term “benign ethnic neutropenia” has been replaced by Duffy-null associated neutrophil count (DANC) (2,4). This terminology shift reflects improved understanding of genetic variations affecting neutrophil counts and avoids misleading or stigmatizing language.
What is Your Approach to Unexplained Neutropenia?
Causes of neutropenia range from benign and transient to serious and malignant, with many possibilities in between. I find it helpful to approach neutropenia by organizing causes according to underlying mechanisms:
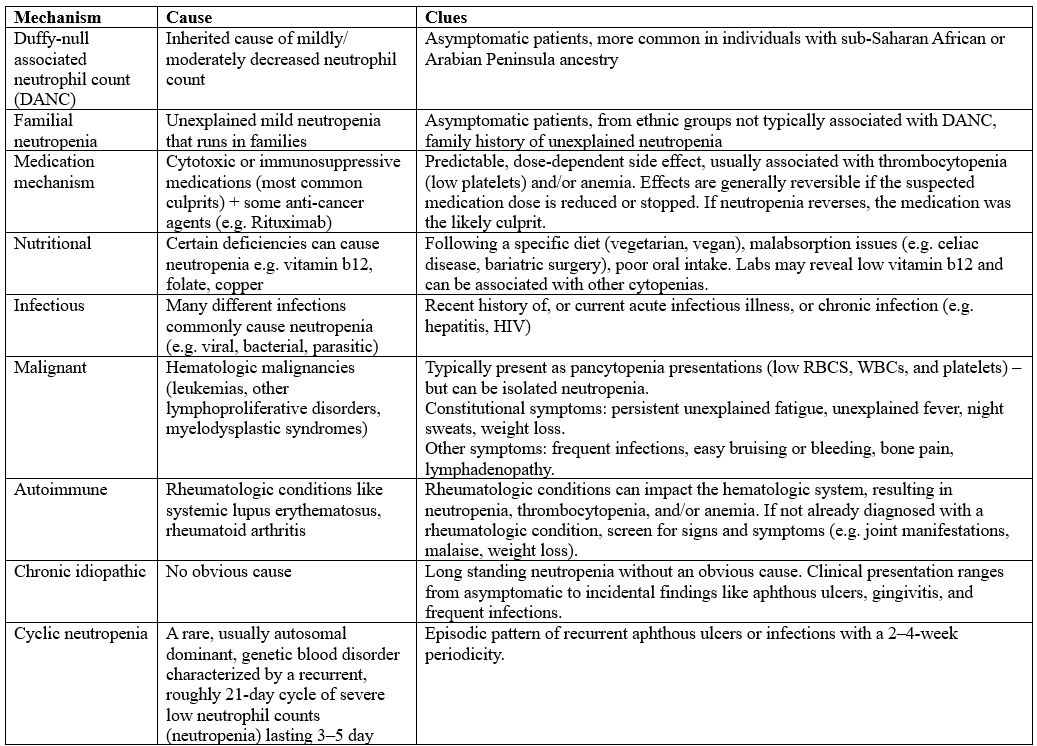
source: (2)
When evaluating an incidental finding of neutropenia, we must determine whether it reflects a benign, transient process or something more serious. A structured history and focused physical exam are essential to guide appropriate follow-up and management.
High-Yield History Tips
Your primary goal is to identify evidence of an underlying disorder that could explain the neutropenia. Let your differential guide your questions. Look for:
Constitutional symptoms: Unexplained fever, severe fatigue, drenching night sweats, unintentional weight loss, recurrent infections, lymphadenopathy ➝ These raise concern for infection, autoimmune disease, or hematologic malignancy.
Cyclic patterns: recurrent aphthous ulcers or infections occurring every 2 to 4 weeks may suggest cyclic neutropenia ➝ concern for cyclic neutropenia
Infectious history: recent viral illness at the time of bloodwork, history of chronic infections (e.g. Hepatitis, HIV), and other infections like Epstein-Barr virus or intestinal parasites. Transient viral suppression is a common cause of mild neutropenia.
Rheumatologic clues: history or symptoms suggestive of autoimmune or connective tissue disease
Medication review: Cytotoxic agents, anti-cancer therapies, immunosuppressants, biologic medications ➝ Medication-induced neutropenia is frequently overlooked.
Nutritional risk factors: restrictive diets, inflammatory bowel disease, celiac disease, history of bariatric surgery ➝ Consider vitamin B12, folate, or copper deficiency.
Hematologic history: personal or family history of neutropenia, history of leukemia, lymphoma, or myelodysplastic syndrome
Ethnicity and genetic considerations: assess ancestry associated with Duffy-null associated neutrophil count (DANC), including Sub-Saharan African ancestry and Arabian Peninsula ancestry (Saudi Arabia, Yemen, Oman, United Arab Emirates, Qatar, Kuwait, and Bahrain) ➝ This distinction is clinically important and helps avoid unnecessary workups (2,3).
Physical Exam Pearls:
Your exam should focus on identifying infection, malignancy, autoimmune disease, or systemic illness.
Signs of infection: fever, cough, myalgias, fatigue, headache, nausea, vomiting, diarrhea, urinary symptoms etc. Even subtle findings matter in neutropenic patients.
Stigmata of liver disease: e.g. Jaundice, ascites, telangiectasias, spider angiomas
Lymphatic and hematologic clues: Lymphadenopathy and splenomegaly. These findings raise concern for hematologic malignancy, other cancers, or rheumatologic conditions.
Musculoskeletal and dermatologic findings: Rash, joint erythema, swelling, or stiffness, aphthous ulcers, gingivitis, angular cheilitis. Recurrent ulcers may suggest cyclic neutropenia. Gingivitis or angular cheilitis may indicate nutritional deficiency.
🚨 Red Flags of Neutropenia
Certain findings warrant urgent evaluation and possible emergency department transfer.
Severe neutropenia
Absolute neutrophil count less than 0.5 × 10³/µL
Concerning smear findings
Leukemic blasts
Nucleated red blood cells
Teardrop cells
Clinical instability
Signs of sepsis
Hemodynamic instability
Respiratory compromise
These patients require urgent specialty evaluation and supportive care (2,3).
Next steps: A reassuring history and exam are helpful, but follow-up labs are still recommended.
Your next step is to determine whether this represents:
Acute or transient neutropenia
Duffy-null associated neutrophil count
Chronic idiopathic neutropenia
Trending counts over time is often the most informative next move (2,3).
Back to the case: We are evaluating a 40-year-old healthy male from Saudi Arabia. He has:
No concerning findings on physical exam
No significant past medical history, including infections, malignancy, autoimmune disease, or nutritional deficiencies
No medication use
So what is the next best step? Before ordering an extensive workup, pause and approach the case systematically.
Unexplained Neutropenia: Lab Test Interpretation
A structured lab review is critical. Start with the basics before expanding your differential.
Step 1: Look for Prior CBC Results
Review any previous CBC with differential counts.
Ask:
Is this new or chronic?
Has the ANC been stable over time?
Is there a downward trend?
Chronic, stable mild neutropenia in an otherwise healthy individual has a very different implication than a new and progressive decline.
Step 2: Assess for Other CBC Abnormalities
If neutropenia occurs alongside other abnormalities, your differential shifts significantly.
Look for:
Anemia
Pancytopenia
Thrombocytopenia
Lymphopenia
Lymphocytosis
Eosinophilia
Basophilia
Isolated neutropenia is reassuring compared with cytopenias affecting multiple cell lines, which raise concern for bone marrow disorders such as myelodysplastic syndrome or hematologic malignancy.
Step 3: The Peripheral Blood Smear
A reflex peripheral smear is often performed automatically when neutropenia is detected. If not, you should order one. A peripheral smear provides essential diagnostic information:
1. Verification: Confirms that the automated analyzer accurately identified a low neutrophil count. Laboratory artifacts can occasionally produce misleading results.
2. Morphology: Evaluates cell size and shape. Abnormal morphology may suggest:
Leukemia
Myelodysplastic syndrome
Other bone marrow pathology
3. Identification of Precursors: Assesses for:
Left shift, meaning increased immature neutrophils, which may indicate acute infection or inflammation
Blast cells, which are primitive undifferentiated cells concerning for acute leukemia
The smear can dramatically narrow your differential before moving to more invasive or costly testing.
Here are some clues to look out for on the peripheral blood smear:
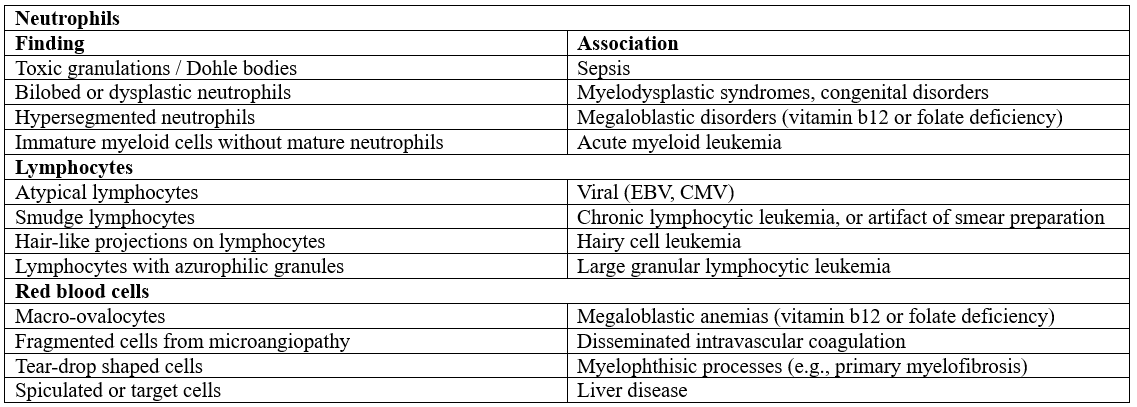
source: 2,3
💡Bottom line: Start with a structure lab test interpretation: Assess the degree of neutropenia (mild, moderate, severe), look for clues on the CBC, differential, and peripheral blood smear that may point towards underlying causes, and assess previous lab trends (normal neutrophil count vs. history of neutropenia).
Managing Isolated Neutropenia
If neutropenia is isolated, management depends on severity and clinical context.
Severe neutropenia: ANC <0.5 x 10³/µL, or other findings like leukemic blasts, nucleated red blood cells, teardrop cells à These patients require urgent assessment and possible hospitalization
The most common cause of severe isolated neutropenia is medication-induced, sepsis, and viral infections.
Moderate neutropenia: >0.5 - <1.0 x 10³/µL, with NO worrisome blood smear findings and NO symptoms: repeat a CBC and differential within 1-2 weeks à if neutropenia persists, follow up as an outpatient
Mild neutropenia: >1.0 x 10³/µL, with NO worrisome blood smear findings and NO symptoms: repeat a CBC and differential within 2-6 weeks à if neutropenia persists, follow up as an outpatient.
The most common causes of mild, isolated neutropenia in adults are DANC, dose-dependent medication-induced, and infections (usually viral). Other causes include nutritional, rheumatologic, and hematologic conditions (e.g. myelodysplasia) (2,3).
Other labs to consider? Additional testing should be guided by your differential and pre-test probability. Avoid shotgun testing and let the clinical picture drive your choices.
Given this patient’s ancestry from Saudi Arabia and lack of clinical red flags, Duffy-null associated neutrophil count remains high on the differential. However, that conclusion should only be reached after appropriate confirmation and exclusion of other causes.
Back to the case: Repeat CBC with differential at one month shows:
ANC 1.2 × 10³/µL
Normal CBC and differential
Normal peripheral smear
He remains asymptomatic. There are no prior CBCs available to demonstrate a previously normal neutrophil count.
What is the most likely diagnosis? DANC – why?
Isolated mild neutropenia
No alternative explanation
No red flags
Saudi Arabian ancestry
This pattern strongly supports DANC.
💡Bottom line: Suspect DANC in patients with mild-moderate isolated neutropenia with reassuring CBC + differential and peripheral blood smear findings, are asymptomatic, and have ancestry associated with DANC.
Should You Order Genetic Testing to Confirm DANC?
Bottom line: not in all cases. In ambiguous presentations, particularly when the ANC is below 1000, ACKR1 gene testing may help confirm Duffy-null status. Routinely ordering genetic testing for patients with an ANC >1000, a classic DANC phenotype presentation, and no clinical features may not represent high-value care. Testing should be targeted to cases where:
The diagnosis remains unclear
Objective confirmation is needed for reassurance
This recommendation is based on expert opinion (4,5).
When to Refer to Hematology
Referral is appropriate when there are features concerning for an underlying hematologic disorder, including:
Severe neutropenia
Abnormal CBC, differential, or peripheral smear findings
Constitutional symptoms like unexplained weight loss, fevers or night sweats
Mucosal findings such as recurrent oral ulcers, recurrent infections (cyclic neutropenia)
Lack of historical or clinical support for DANC
For example, if prior white blood cell counts were consistently normal, referral may be warranted (this is based on expert opinion) (4).
🧪 For weekly lab test interpretation pearls, practical prescribing tips, and practice-changing insights, join NP Reasoning Masterclass.
References/Resources
Choosing Wisely Canada. Ordering routine blood work [Internet]. Toronto (ON): Choosing Wisely Canada; n.d. [cited 2026 Feb 23]. Available from: https://choosingwiselycanada.org/toolkit/ordering-routine-blood-work/
Berliner N. Approach to the adult with unexplained neutropenia [Internet]. In: Post TW, editor. UpToDate. Waltham (MA): UpToDate Inc.; 2026 [cited 2026 Feb 23]. Available from: https://www.uptodate.com/contents/approach-to-the-adult-with-unexplained-neutropenia
Tahir N, Zahra F. Neutrophilia [Internet]. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025 Jan– [updated 2023 Apr 27; cited 2026 Feb 23]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK570571/
Wurtz P, Beeler B, Williams PN, Watto MF. 491 Benign Hematology with Brad Beeler [Internet]. The Curbsiders Internal Medicine Podcast. 2025 Jul 14 [cited 2026 Feb 23]. Available from: https://thecurbsiders.com/category/curbsiders-podcast
Oyogoa E, Mathews R, Olson S, DeLoughery T, Shatzel JJ, Martens KL. Clinical outcomes of patients referred for asymptomatic neutropenia: A focus on racial disparities in hematology. Eur J Haematol. 2023 Jul;111(1):41-46. doi:10.1111/ejh.13963. PMID: 36951011; PMCID: PMC10272056.
Sohail H, Collins JE, Chan KH, Alamgir MA, Kamran AS. A retrospective, real-world study of IV iron use to treat iron deficiency anemia during acute infection. Blood. 2026 Jan 27:blood.2025031965. doi:10.1182/blood.2025031965. Epub ahead of print. PMID: 41592284.
Hibbs SP, Chipare I, Halawani AJ, Legge SE, Fell G, Dees D, et al. Multinational assessment of absolute neutrophil counts and white blood cell counts among healthy Duffy-null adults. Blood. 2026 Jan 15;147(3):290-298. doi:10.1182/blood.2025029359. PMID: 41191521.