

Multiple Sclerosis Diagnosis: MRI Findings, Imaging Protocols, and Interpretation Pearls for Clinicians
Multiple sclerosis can be a sneaky disease. It does not always present typically, findings can be subtle, and in relapsing-remitting disease, symptoms may disappear for months or even years. In this post, we provide a focused overview of multiple sclerosis, with an emphasis on diagnostic imaging essentials and interpretation pearls for clinical practice. First, let’s anchor our learning to a case:
Case: A 30-year-old male presents with right hand weakness for the past 12 months. He is right-hand dominant and reports reduced grip strength. He also describes intermittent double vision over the past 6 months, which he attributed to stress. He denies diplopia today.
He takes amlodipine for hypertension. His blood pressure today is 125/85. On examination, grip strength is 4/5 on the right and 5/5 on the left. There are no other focal neurological deficits. He is otherwise healthy.
What do you make of this presentation? What illness scripts does it trigger?
Motor weakness combined with visual symptoms raises several possibilities, including one diagnosis we do not want to miss: multiple sclerosis.
What Is Multiple Sclerosis?
Multiple sclerosis (MS) is a chronic autoimmune-mediated inflammatory and neurodegenerative disease of the central nervous system. It is characterized by demyelination, which is destruction of the myelin sheath surrounding nerve fibers, and axonal transection, which is severing of nerve fibers. Together, these processes lead to progressive neurological disability (1,2).
Epidemiology and Risk Factors of Multiple Sclerosis
MS affects approximately 900,000 people in the United States and 2.8 million worldwide (1,3). It typically presents in young adults between ages 20 and 30 and affects women about three times more often than men (1). Life expectancy is reduced compared to the general population, with averages of 75.9 versus 83.4 years (1).
The cause of MS remains unclear but involves a combination of genetic and environmental factors. Key contributors include:
Genetic predisposition plays a major role, with the HLA-DRB1*15:01 allele being the strongest known risk factor, conferring an odds ratio of approximately 3. First-degree relatives have a 2-4 % risk compared to 0.1 percent in the general population, and monozygotic twin concordance ranges from 30-50% (1,4).
Epstein-Barr virus infection is now considered a necessary, though not sufficient, cause of MS, with seroconversion preceding disease onset (5).
Environmental factors also contribute. Vitamin D deficiency and low sun exposure are associated with higher prevalence at temperate latitudes. Smoking increases risk with a relative risk of about 1.5, and childhood or adolescent obesity carries a hazard ratio of approximately 1.6 (1,4).
Pathophysiology of Multiple Sclerosis
MS lesions are characterized by focal areas of demyelination and inflammation, primarily affecting white matter, although grey matter and cortical lesions are also common (1).
The disease process involves several key steps. Autoreactive T cells and B cells cross the blood-brain barrier, leading to inflammatory infiltration. This results in demyelination and oligodendrocyte injury. Axonal transection follows, representing irreversible neurological damage. Lesions may subsequently remyelinate, resolve, or persist in a chronic inflammatory state (2,6).
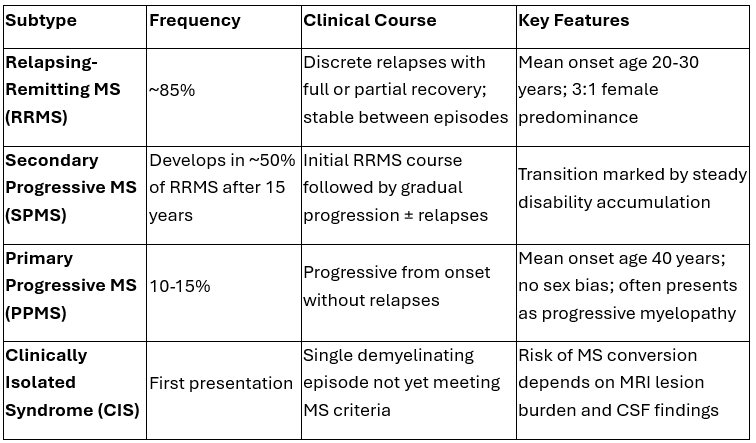
Clinical subtypes of Multiple sclerosis
Current classification also incorporates disease activity and progression, allowing for more precise phenotyping.
Sources: 1-4
Prognosis of Multiple Sclerosis
Factors associated with a higher likelihood of progression include older age at onset, high or persistent inflammatory activity, extensive spinal cord or cortical lesion burden, impaired repair capacity, mitochondrial dysfunction, and delayed treatment initiation.
Conversely, younger age, lower inflammatory burden, minimal spinal cord involvement, robust repair mechanisms, and early treatment are associated with a more favorable course.
Signs and Symptoms: When to Suspect Multiple Sclerosis
MS should be suspected when patients present with focal neurological symptoms that evolve over hours to days rather than suddenly, as in stroke.
Typical features include onset between ages 20 and 40, symptoms referable to central nervous system white matter tracts such as the optic nerve, spinal cord, brainstem, or cerebellum, and a relapsing-remitting pattern (the most common) with episodes lasting more than 24 hours followed by recovery.
Objective neurological findings may include an afferent pupillary defect, hyperreflexia, extensor plantar response, ataxia, or a sensory level (a distinct horizontal line on the body below which sensation is diminished, indicating a transverse myelitis or significant spinal cord lesion (7).
Bottom line: Suspect MS in young adults with focal central nervous system symptoms developing over days with spontaneous recovery (note: primary progressive MS typically is not characterized by spontaneous recovery).
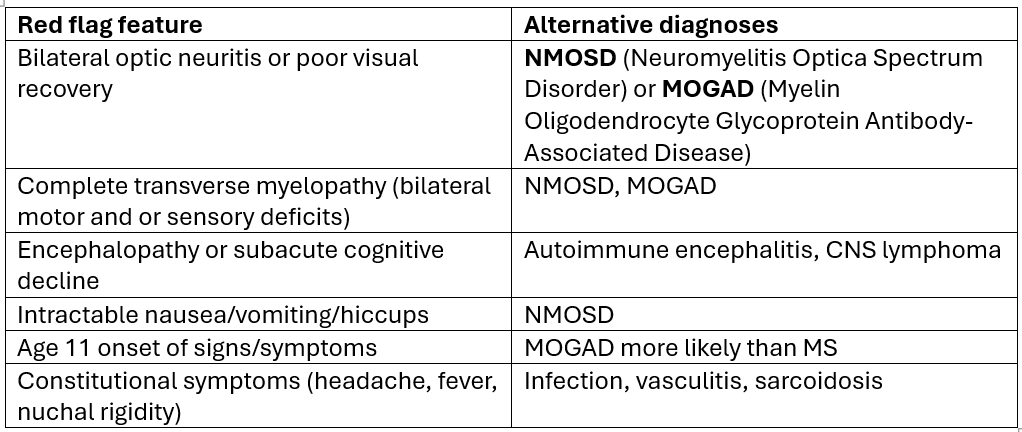
Differential Diagnosis and Red Flags in Suspected MS
Even when MS is suspected, alternative diagnoses must be considered, especially in the presence of red flags.
Sources: 1, 7, 8
MRI in Multiple Sclerosis: What to Order and Why
Recommended MRI Protocol
MRI is the cornerstone of MS diagnosis.
Order an MRI of the brain without and with gadolinium contrast in all patients with suspected MS.
MRI of the cervical and thoracic spine without and with contrast is recommended when brain imaging is non-diagnostic, when myelopathy is suspected, or when additional diagnostic confidence is needed (10,11).
Why Spinal Cord Imaging Matters
Spinal cord lesions are present in 80-90% of patients with established MS and in 30-50 % of those with clinically isolated syndrome (8).
Importantly, spinal cord lesions do not occur with normal aging or typical cerebrovascular disease, making them highly specific for MS and extremely useful diagnostically (12). The presence of multiple peripheral, asymmetric spinal cord lesions is highly characteristic of MS (12).
Bottom line: Order brain MRI with contrast first. Add spinal imaging if needed or when suspicion is moderate to high. Ordering both upfront is reasonable in many cases.
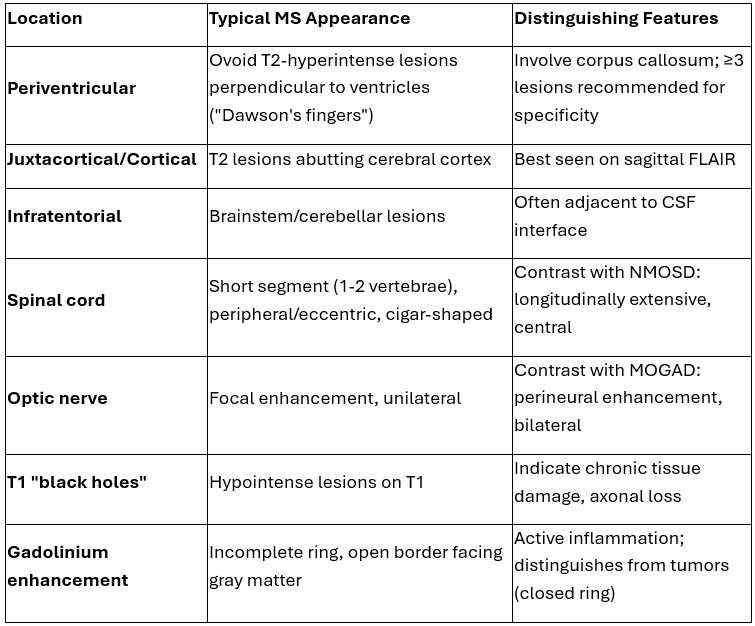
Characteristic Findings of Multiple Sclerosis on MRI
Sources: 10-12
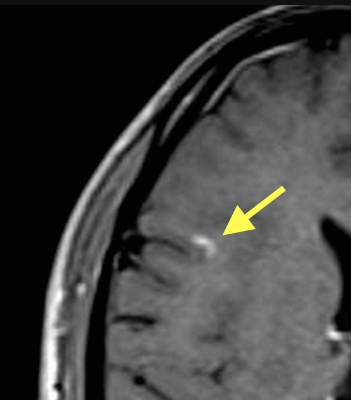
Right frontal lobe enhancing juxtacortical lesion. Source: Radiopedia
Bottom line: Look for periventricular, juxtacortical, infratentorial, and spinal cord lesions on T2 imaging. Gadolinium enhancement indicates active disease.
Back to the case: subsequent MRI of the brain and cervical spine confirms the diagnosis.
Brain imaging demonstrates multiple ovoid T2 hyperintense lesions in the periventricular region, oriented perpendicular to the lateral ventricles, consistent with Dawson’s fingers. Additional lesions are seen in the juxtacortical region and corpus callosum. Some lesions show gadolinium enhancement, indicating active inflammation.
Cervical spine imaging reveals short segment, peripheral T2 hyperintense lesions without longitudinal extension, further supporting the diagnosis of MS over alternative demyelinating conditions.
Next steps: neurology referral.
Key Takeaway for primary care
Multiple sclerosis is often subtle and easily missed. Early recognition depends on identifying characteristic clinical patterns and understanding how to interpret MRI findings.
If you suspect MS, order the appropriate imaging early and look for lesions in the right locations. When the clinical picture and imaging align, timely referral and treatment can significantly alter the disease course.
💡For weekly diagnostic imaging insights and practice-changing pearls, join NP Reasoning Masterclass.
ReferencesMcGinley MP, Goldschmidt CH, Rae-Grant AD. Diagnosis and treatment of multiple sclerosis: a review. JAMA. 2021;325(8):765-779. doi:10.1001/jama.2020.26858Rida ZS, Zeb Khan J, Khalid Tipu M, Jahan F, Irshad N. A review on multiple sclerosis: unravelling the complexities of pathogenesis, progression, mechanisms and therapeutic innovations. Neuroscience. 2025;567:133-149. doi:10.1016/j.neuroscience.2024.12.029Tramacere I, Virgili G, Perduca V, Lucenteforte E, Benedetti MD, Capobussi M, et al. Adverse effects of immunotherapies for multiple sclerosis: a network meta-analysis. Cochrane Database Syst Rev. 2023;11:CD012186. doi:10.1002/14651858.CD012186.pub2Reich DS, Lucchinetti CF, Calabresi PA. Multiple sclerosis. N Engl J Med. 2018;378(2):169-180. doi:10.1056/NEJMra1401483Aloisi F, Giovannoni G, Salvetti M. Epstein-Barr virus as a cause of multiple sclerosis: opportunities for prevention and therapy. Lancet Neurol. 2023;22(4):338-349. doi:10.1016/S1474-4422(22)00471-9Faissner S, Plemel JR, Gold R, Yong VW. Progressive multiple sclerosis: from pathophysiology to therapeutic strategies. Nat Rev Drug Discov. 2019;18(12):905-922. doi:10.1038/s41573-019-0035-2Saguil A, Farnell EA 4th, Jordan TS. Multiple sclerosis: a primary care perspective. Am Fam Physician. 2022;106(2):173-183.Kalnins A, Lewis L, Soderlund K, et al. ACR Appropriateness Criteria® demyelinating diseases. J Am Coll Radiol. 2026.Brownlee WJ, Hardy TA, Fazekas F, Miller DH. Diagnosis of multiple sclerosis: progress and challenges. Lancet. 2017;389(10076):1336-1346. doi:10.1016/S0140-6736(16)30959-XBarkhof F, Reich DS, Oh J, Rocca MA, Li DKB, Sati P, et al. 2024 MAGNIMS-CMSC-NAIMS consensus recommendations on the use of MRI for the diagnosis of multiple sclerosis. Lancet Neurol. 2025;24(10):866-879. doi:10.1016/S1474-4422(25)00304-7Traboulsee A, Ontaneda D, Rovira À, et al. Magnetic resonance imaging in multiple sclerosis: consensus guidelines from MAGNIMS, CMSC, and NAIMS. Lancet Neurol. 2025;24(10):866-879. doi:10.1016/S1474-4422(25)00304-7Ciccarelli O, Cohen JA, Reingold SC, Weinshenker BG. Spinal cord involvement in multiple sclerosis and neuromyelitis optica spectrum disorders. Lancet Neurol. 2019;18(2):185-197. doi:10.1016/S1474-4422(18)30460-5