

Palpitations Workup: ECG, Holter Monitor, Echocardiogram, and Stress Tests Explained
Palpitations: How to Choose the Right Cardiac Test
Palpitations are a common yet often challenging presentation in primary care. While many cases are benign, others may signal significant arrhythmia or structural heart disease. The key lies in knowing how to risk stratify and select the right cardiac test.
First, let’s start with a case to anchor our learning.
Case: You are seeing a 65-year-old male presents with intermittent fluttering in his chest over the past month. Episodes occur at rest and during activity, seemingly at random, and last between 1 and 5 minutes. Occasionally, they wake him from sleep.
He denies chest pain, diaphoresis, shortness of breath, weakness, or syncope.
You suspect palpitations. What is your approach?
Approach to Palpitations: Cardiac vs Non-Cardiac Causes
A helpful framework I like to use is to divide differentials into cardiac and non-cardiac etiologies:
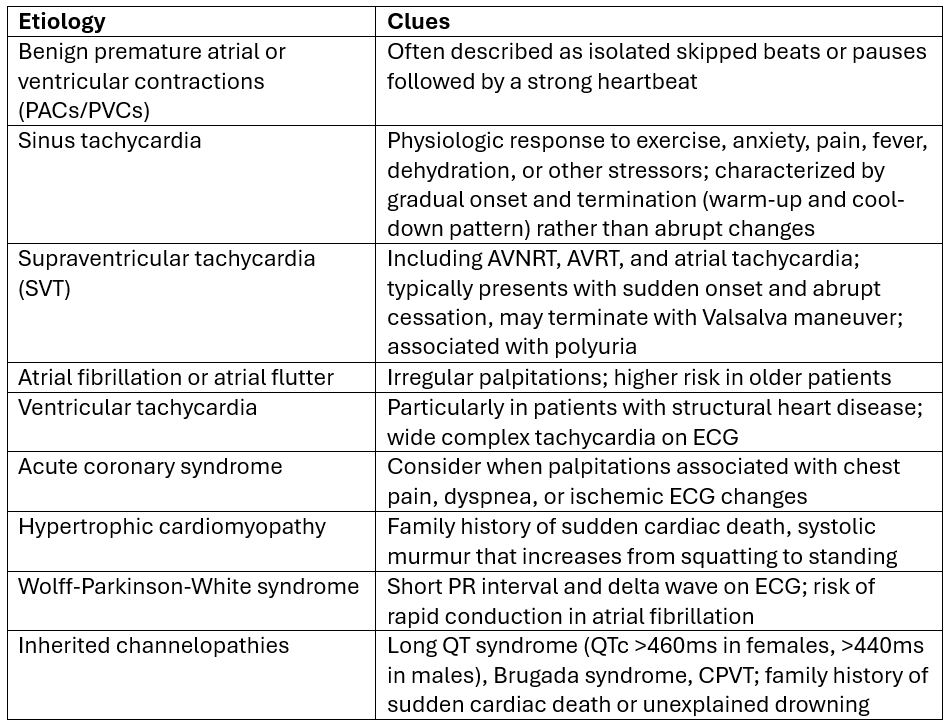
source: 1
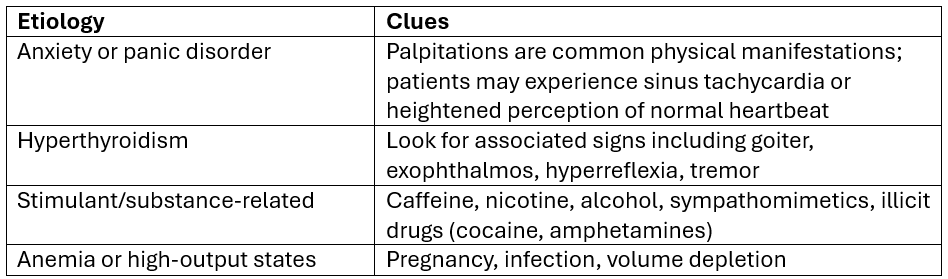
source: 1
Back to the case: On further assessment, the patient remains hemodynamically stable. His cardiovascular exam is normal, but the history is concerning for an intermittent arrhythmia given the episodic nature, nocturnal symptoms, and lack of clear triggers.
This is not a presentation you can confidently dismiss as benign. Cardiac testing is warranted.
Cardiac Testing for Palpitations: ECG and Beyond
Electrocardiogram (ECG): First-Line Test
What it’s for: the initial test for all patients presenting with palpitations. It can identify arrhythmias, ischemia, conduction abnormalities, and syndromic conditions such as Wolff-Parkinson-White or long QT syndrome.
However, its diagnostic yield depends heavily on timing. When performed outside of symptoms, sensitivity is low, with yields ranging from 3-26%. This increases to approximately 48% if obtained during active palpitations (1).
A normal ECG does not rule out arrhythmia. False negative results is a key limitation. Many arrhythmias are intermittent, and the ECG simply captures a brief moment in time. However, the ECG remains valuable for identifying structural abnormalities (WPW, long QT, Brugada pattern, LVH) and baseline conduction disorders that increase arrhythmia risk (1).
False positives are uncommon but can occur due to artifact from movement, tremor, or poor electrode contact. Interpretation accuracy is also slightly lower in non-specialist settings (2).
Holter Monitoring and Extended Cardiac Monitoring
What it’s for: primarily ordered for palpitations to establish symptom-rhythm correlation and diagnose the underlying arrhythmia in patients experiencing daily or near-daily symptoms. The key purpose is to capture the cardiac rhythm during symptomatic episodes to determine whether palpitations are caused by an arrhythmia and, if so, to identify the specific type.
Holter monitoring between 24-72 hours is best suited for patients with daily or very frequent symptoms. The diagnostic yield is modest, around 10-15%, largely because symptoms may not occur during the monitoring window (1,3).
Longer monitoring significantly improves detection, especially if patients have more sporadic symptoms. A 14-day patch monitor offers the highest yield-to-cost ratio, with detection rates up to 70-85% for unexplained palpitations (1).
Extended monitoring consistently outperforms short-duration Holter monitoring. For example, detection rates for arrhythmias may reach nearly 60% with 14-day monitoring compared to about 19% with 24-hour Holter (4)
Limitations: increased sensitivity comes with trade-offs. A large proportion of detected arrhythmias are asymptomatic, which can lead to overdiagnosis of benign ectopy (5).
Technical limitations also exist. Poor signal quality, motion artifact, and algorithm limitations can result in false positives or missed events (5).
Bottom line: Use Holter monitoring for frequent symptoms and consider extended monitoring for intermittent episodes.
Echocardiography: When to Look for Structural Disease
What it’s for: Echocardiography is not a screening test but a targeted investigation. It’s indicated if there are abnormal physical exam findings such as a new murmur, signs of heart failure, abnormal ECG findings, syncope or presyncope, or a family history of cardiomyopathy or sudden cardiac death. They are primarily ordered in the context of palpitations to detect underlying structural heart disease that may predispose to arrhythmias or directly cause palpitations. The key purpose is risk stratification rather than rhythm diagnosis—echocardiography identifies cardiac substrates that increase the risk of serious arrhythmias and helps guide management decisions.
Strengths: identifying structural abnormalities. It performs significantly better than clinical examination alone in detecting left ventricular dysfunction and valvular disease (6).
In symptomatic patients referred from primary care, approximately one in four will have findings that may change management, many of which are new diagnoses.
Limitations: Echocardiography has excellent specificity for structural abnormalities when present, but sensitivity is limited for detecting ischemia without active symptoms. Segmental wall motion abnormalities can occur in both ischemic and non-ischemic cardiomyopathies, reducing specificity for CAD (6).There may also be technical challenges related to patient body habitus or lung disease.
Bottom line: Reserve echocardiography for patients with abnormal exam findings, ECG abnormalities, syncope, or relevant family history (i.e. when structural heart disease is suspected).
Exercise Stress Testing: When Ischemia Is Suspected
What it’s for: Exercise stress testing is most useful for patients with exertional symptoms or suspected coronary artery disease.
Its diagnostic accuracy is modest. Sensitivity averages around 68% and specificity around 77%, though real-world sensitivity may be lower (7).
Limitations: False negatives are common, especially in patients with single-vessel disease, those on anti-ischemic medications, or those unable to achieve target heart rate. False positives may occur due to baseline ECG abnormalities, electrolyte disturbances, or other non-ischemic factors (5).
Importantly, test performance depends heavily on pretest probability. In low-risk patients, false positives are common. In high-risk patients, false negatives are more concerning (8).
Compared with other modalities, exercise ECG has lower diagnostic accuracy than stress echocardiography or cardiac MRI.
Bottom line: consider stress testing when symptoms are exertional or when ischemia is suspected.
Red Flags vs Low-Risk Features in Palpitations
Certain features should prompt urgent referral to the emergency department and cardiology consultation:
Hemodynamic instability
Ischemic chest pain
Syncope or presyncope
Palpitations during exertion
Family history of sudden cardiac death
Resting tachycardia above 120 beats per minute
Wide complex tachycardia
High-grade heart block
ECG findings suggestive of channelopathies or ischemia
In contrast, low-risk patients typically have isolated palpitations without associated symptoms, no structural heart disease, no concerning family history, and a normal ECG (1).
Back to the case: The patient’s ECG is normal. However, given the intermittent nature of his symptoms and the known false negative rate of ECGs performed outside of episodes, your pretest probability for arrhythmia remains intermediate.
Because his symptoms occur every 1-2 days, you order a 48-hour Holter monitor.
The Holter captures the following: paroxysmal atrial fibrillation, confirming the diagnosis and guiding next steps in management.
Clinical Bottom Lines for Primary Care
A sequential, risk-based testing strategy is key for palpitation presentations.
Start with an ECG, ideally during symptoms when possible.
Be mindful of overdiagnosis. Extended monitoring often detects asymptomatic ectopy that may not explain the patient’s symptoms and can lead to unnecessary intervention.
💡For weekly diagnostic imaging insights and practice-changing pearls, join NP Reasoning Masterclass.
ReferencesGauer RL, Thomas MF, McNutt RA. Palpitations: evaluation, management, and wearable smart devices. Am Fam Physician. 2024;110(3):259-269.US Preventive Services Task Force. Screening for atrial fibrillation: US Preventive Services Task Force recommendation statement. JAMA. 2022;327(4):360-367. doi:10.1001/jama.2021.23732Steinberg JS, Varma N, Cygankiewicz I, et al. 2017 ISHNE-HRS expert consensus statement on ambulatory ECG and external cardiac monitoring/telemetry. Heart Rhythm. 2017;14(7):e55-e96.Liu CM, Chang SL, Yeh YH, Chung FP, Hu YF, Chou CC, et al. Enhanced detection of cardiac arrhythmias utilizing 14-day continuous ECG patch monitoring. Int J Cardiol. 2021;332:78-84. doi:10.1016/j.ijcard.2021.03.015Kadish AH, Buxton AE, Kennedy HL, et al. ACC/AHA clinical competence statement on electrocardiography and ambulatory electrocardiography: a report of the ACC/AHA/ACP-ASIM Task Force on Clinical Competence. J Am Coll Cardiol. 2001;38(7):2091-2100. doi:10.1016/S0735-1097(01)01680-1Greenland P, Alpert JS, Beller GA, Benjamin EJ, Budoff MJ, Fayad ZA, et al. 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2010;56(25):e50-e103. doi:10.1016/j.jacc.2010.09.001Singh T, Bing R, Dweck MR, et al. Exercise electrocardiography and computed tomography coronary angiography for patients with suspected stable angina pectoris: a post hoc analysis of the randomized SCOT-HEART trial. JAMA Cardiol. 2020;5(8):920-928. doi:10.1001/jamacardio.2020.1567Morise AP. Are the American College of Cardiology/American Heart Association guidelines for exercise testing for suspected coronary artery disease correct? Chest. 2000;118(2):535-541. doi:10.1378/chest.118.2.535