

Microscopic Hematuria: A Practical, Stepwise Approach for Primary Care
Microscopic hematuria is one of those findings that’s easy to overlook—and just as easy to over-investigate. The challenge in primary care is knowing when it matters, what to rule out, and how far to go.
Let’s walk through a practical, evidence-informed approach you can actually use in clinic.
🔎Case: You’re following up a 50-year-old man with irritative voiding symptoms (urgency, frequency). Initial urinalysis shows red blood cells, but urine culture is negative. Repeat urine microscopy reveals 5 RBCs per high-power field (HPF).
What is Microscopic Hematuria?
Microscopic hematuria is defined as: >3 RBCs per HPF on a properly collected urine specimen (1).
A key clinical point:
A positive dipstick alone is not enough
Dipsticks have false positives
Always confirm with urine microscopy (urine R&M) (1)
Differential Diagnosis of Microscopic Hematuria
Microscopic hematuria spans a wide spectrum, from benign to life-threatening.
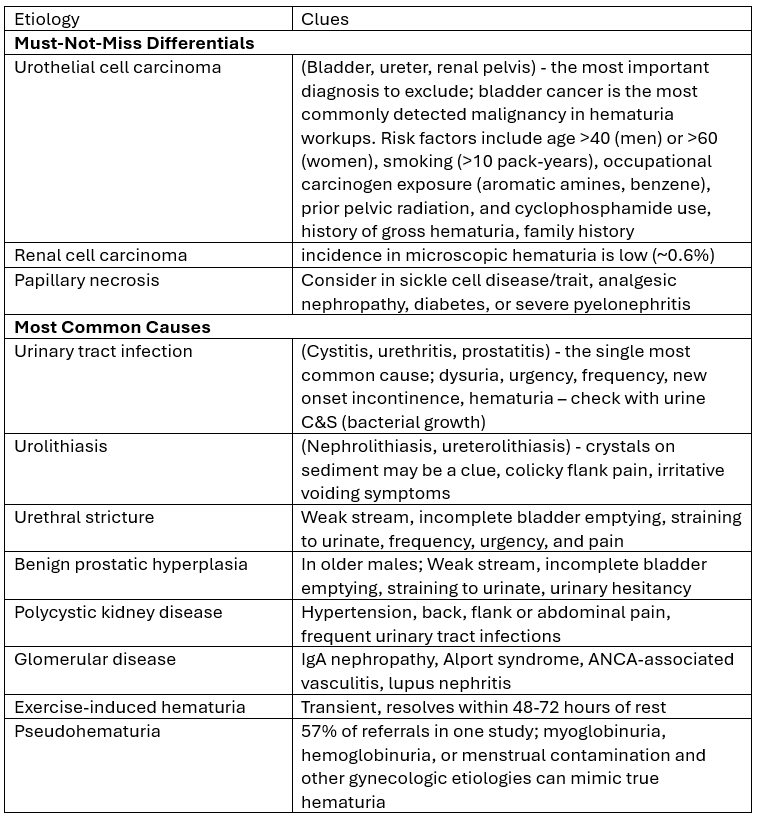
Sources: 1-7
An early and important step is figuring out where the bleeding is coming from: glomerular or non-glomerular.
Glomerular hematuria points to pathology within the glomeruli, often due to immunologic, inflammatory, or metabolic disease. Think conditions like lupus nephritis or diabetic kidney disease. This is often accompanied by proteinuria (7,8).
Non-glomerular hematuria reflects pathology outside the glomeruli, including the renal tubules, vasculature, or the broader urinary tract. Common causes include infection, stones, tumors, or structural abnormalities (7,8).
We’ll come back to some high-yield lab clues that help distinguish between these two.
First, let’s get into some high-yield history questions and physical exam pearls to further narrow down your differential.
💡 Bottom line: Microscopic hematuria is >3 RBCs per HPF on a properly collected urine specimen - always confirm with 2 urine routine and microscopy tests.
High-Yield History Questions
A focused history will often point you in the right direction before any additional testing.
Start with urinary symptoms: dysuria, urgency, frequency, hesitancy, incomplete emptying, or straining. These help screen for infection, BPH, or urethral stricture.
Ask about recent exercise, especially around the time of the urine sample. Transient hematuria after vigorous activity is common and easily missed.
Consider a gynecologic source when relevant. Clarify timing with menstruation, symptoms of genitourinary syndrome of menopause, and any signs of vulvovaginitis such as unusual discharge. Also ask about recent procedures like IUD insertion, endometrial biopsy, or even a pelvic exam.
Screen for urolithiasis with colicky flank or groin pain, along with nausea, vomiting, urgency, frequency, or dysuria.
Don’t forget malignancy risk factors. A smoking history >10 pack-years, occupational exposures (such as aromatic amines or benzene), prior pelvic radiation, and cyclophosphamide use all increase concern.
Round it out with past medical history, including diabetes, sickle cell disease, autoimmune conditions like lupus, polycystic kidney disease, and prior kidney stones.
Physical Exam Pearls
A targeted physical exam can help distinguish benign from more serious causes.
Check vital signs, especially for hypertension, which may suggest glomerular disease.
Look for peripheral edema or rashes, raising concern for systemic or vasculitic processes.
Perform a pelvic exam if a gynecologic source is suspected.
In males, consider a digital rectal exam if a prostatic cause is on the table.
Include an external genital exam to assess for urethral discharge, irritation, or trauma if indicated.
On abdominal exam, assess for masses, organomegaly, or tenderness.
Finally, check for costovertebral angle tenderness, which may point toward kidney involvement such as infection or stones.
Before moving on to additional investigations, make sure you’ve excluded common transient causes such as urinary tract infection, menstruation, and recent vigorous exercise. Once these are ruled out, it’s time to proceed with further lab evaluation.
🔎 Back to the Case: there are no identifiable transient causes (exercise, menstruation, infection), and she is not yet menopausal. On a careful history and physical exam there is no obvious underlying cause for the microscopic hematuria. What’s next?
Diagnostic Approach to Microscopic Hematuria
Once you’ve confirmed microscopic hematuria, the lab workup should be deliberate and efficient. Here’s a clean, stepwise approach you can use in practice:
Step 1) Confirm it’s real: Microscopic hematuria is defined as >3 RBCs per HPF. Confirm the presence of microscopic hematuria with a repeat a urine routine and microscopy (urine R&M). Persistent findings on repeat testing confirm true microscopic hematuria (1).
Step 2) Look for glomerular clues: Examine the urine sediment carefully. Dysmorphic RBCs, casts, and proteinuria all point toward a glomerular source. If these are present, shift your thinking toward intrinsic kidney disease. This should prompt further workup, including serum creatinine, urine ACR, complement levels, and autoimmune serologies, along with a nephrology referral. Some patients may ultimately require renal biopsy (1).
Step 3) Check kidney function in everyone: Order serum creatinine and urine ACR regardless of the suspected source. Even if you think this is urologic, you don’t want to miss underlying kidney disease or clinically significant proteinuria (1).
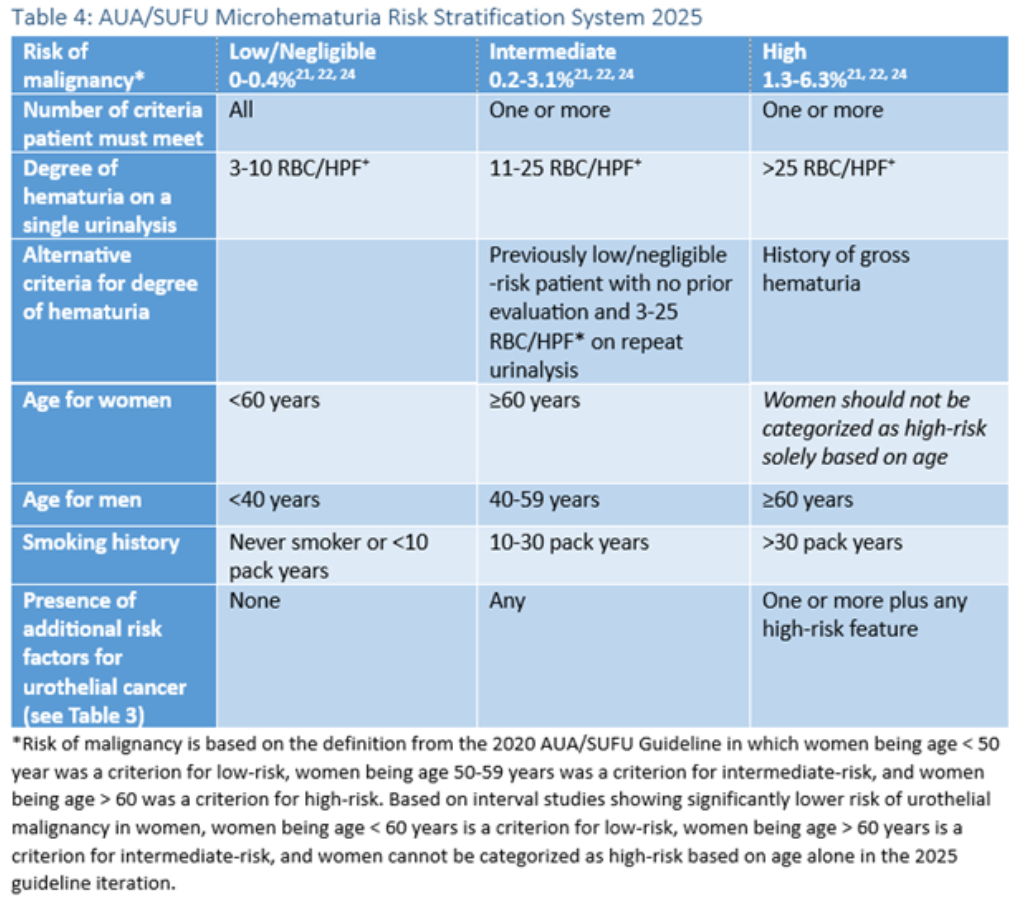
Step 4) Risk-stratify for malignancy: Not all microscopic hematuria needs the same intensity of workup. Use the 2025 AUA/SUFU Microhematuria Risk Stratification System to guide next steps. This framework incorporates age, sex, smoking history, degree of hematuria, and other risk factors to help determine who needs imaging and cystoscopy (1).
Step 5) Target your additional workup: From here, tailor investigations based on your leading differential. For example, evaluate for BPH, stones, or polycystic kidney disease if clinically suspected. The goal is to stay focused rather than ordering a broad, unfocused panel.
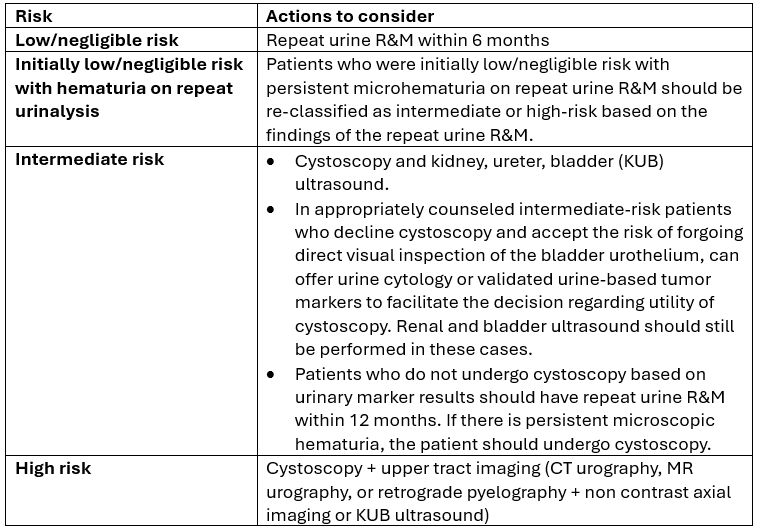
🔎Back to the Case: Back to the case: On repeat urine R&M the results are 15 RBC/HPF. She has a history of 20 pack years of smoking cigarettes. These 2 factors would place her in “intermediate” risk for malignancy.
Next steps: KUB ultrasound and cystoscopy (referral to a specialist for the latter).
And as always, when in doubt - consult a specialist.
💡 Bottom line: Risk stratification for malignancy is key to determine the next steps in evaluating your patient with microscopic hematuria.
Imaging in Microscopic Hematuria: Ultrasound vs CT Urography
Imaging plays a key role in evaluation, but not all modalities are created equal.
Renal Cell Carcinoma: Ultrasound Performs Reasonably Well
For renal cell carcinoma, ultrasound performs reasonably well. In the DETECT I study, it demonstrated a sensitivity of 85.7% and a negative predictive value of 99.9% (9). Missed cancers tend to be small and early-stage (11). Contrast-enhanced ultrasound can improve lesion characterization, but it is not routinely used in hematuria workups (12–14).
Upper Tract Urothelial Carcinoma: The Major Limitation of Ultrasound
However, ultrasound performs poorly for upper tract urothelial carcinoma. Sensitivity ranges from 14% to 33%, compared with 80% to 99% for CT urography (15,16). This represents the major limitation of ultrasound in this setting. In the DETECT I study, sensitivity for UTUC was just 14.3% (9).
Bladder Cancer: Imaging Has Limits
For bladder cancer, ultrasound is again limited, with sensitivity between 35% and 51%. Cystoscopy remains the gold standard for evaluating the lower urinary tract (9,16).
Clinical Implications
The AUA/SUFU 2025 guidelines recommend renal ultrasound for intermediate-risk patients, reflecting the relatively low prevalence of upper tract malignancy (approximately 0.3–0.6%). In these patients, the balance of benefits and harms favors ultrasound over CT (1).
CT urography is reserved for high-risk patients, where its higher sensitivity justifies the increased radiation exposure, contrast use, and cost (15).
💡 Bottom line: KUB ultrasound performs reasonably well for renal cell carcinoma but is poor for upper tract urothelial carcinoma. For intermediate-risk patients, KUB US is recommended. For high-risk patients, CT urography is the gold standard.
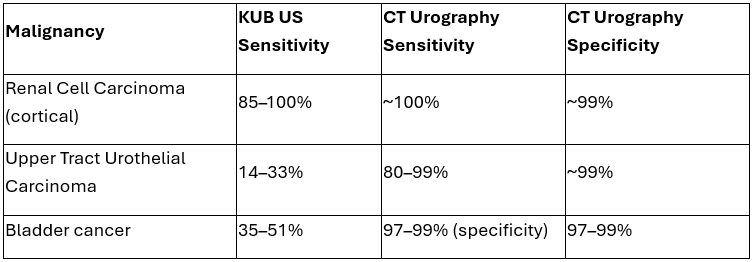
Summary of diagnostic imaging test accuracy for malignancy evaluation in microscopic hematuria
Microscopic hematuria is common, but the stakes can be high. The goal is not to investigate everyone aggressively, but to identify who needs further evaluation. A practical approach is simple:
Confirm → Localize the source → Risk-stratify → Investigate
Done well, this approach helps you catch serious disease without over-investigating low-risk patients.
✨ Join NP Reasoning for weekly lab test pearls & updates ✨
ReferencesBarocas DA, Lotan Y, Matulewicz RS, Raman JD, Westerman ME, Kirkby E, Pak L, Souter L. Updates to microhematuria: AUA/SUFU guideline (2025). J Urol. 2025;213(5):547-557. doi:10.1097/JU.0000000000004490.Arnold MJ. Microscopic hematuria in adults: Updated recommendations from the American Urological Association. Am Fam Physician. 2021;104(6):655-657.Sharp VJ, Barnes KT, Erickson BA. Assessment of asymptomatic microscopic hematuria in adults. Am Fam Physician. 2013;88(11):747-754.Cohen RA, Brown RS. Microscopic hematuria. N Engl J Med. 2003;348(23):2330-2338. doi:10.1056/NEJMcp012694.Udedibia E, Solosky K, Macdonald EJ, et al. Critical analysis of the AUA 2020/2025 microscopic hematuria guidelines to predict urothelial but not renal cortical neoplasms. J Urol. 2026;215(4):441-449. doi:10.1097/JU.0000000000004854.Rai BP, Dominguez Escrig JL, Vale L, et al. Systematic review of the incidence of and risk factors for urothelial cancers and renal cell carcinoma among patients with haematuria. Eur Urol. 2022;82(2):182-192. doi:10.1016/j.eururo.2022.03.027.Saha MK, Massicotte-Azarniouch D, Reynolds ML, et al. Glomerular hematuria and the utility of urine microscopy: A review. Am J Kidney Dis. 2022;80(3):383-392. doi:10.1053/j.ajkd.2022.02.022.Ronco P, Rovin B, Schiandorf D, et al. The 2021 clinical practice guideline for the management of glomerular diseases. Kidney Int. 2021.Smith MR, Read KC, Stegman ML, Kroll NJ, Van Every MJ. Evaluation of asymptomatic microscopic hematuria by renal ultrasound to detect upper tract malignancy: A 20-year experience. Urology. 2019;133:34-39. doi:10.1016/j.urology.2019.07.009.1Bochner E, Ibezue C, Banerji D, et al. Assessing the diagnostic performance of renal ultrasound in microhematuria evaluation. Urology. 2025;S0090-4295(25)00881-7. doi:10.1016/j.urology.2025.09.012.Zhang F, Li R, Li G, et al. Value of contrast-enhanced ultrasound in the diagnosis of renal cancer compared with CT: A meta-analysis. J Ultrasound Med. 2019;38(4):903-914. doi:10.1002/jum.14769.Wang C, Yu C, Yang F, Yang G. Diagnostic accuracy of contrast-enhanced ultrasound for renal cell carcinoma: A meta-analysis. Tumour Biol. 2014;35(7):6343-6350. doi:10.1007/s13277-014-1815-2.Pan KH, Jian L, Chen WJ, et al. Diagnostic performance of contrast-enhanced ultrasound in renal cancer: A meta-analysis. Front Oncol. 2020;10:586949. doi:10.3389/fonc.2020.586949.Taylor JI, Souter LH, Barocas DA, et al. Diagnostic imaging in the evaluation of asymptomatic microhematuria: Systematic review and meta-analysis. J Urol. 2023;209(6):1099-1106. doi:10.1097/JU.0000000000003395.Fankhauser CD, Waisbrod S, Fierz C, et al. Diagnostic accuracy of ultrasonography, CT, cystoscopy and cytology to detect urinary tract malignancies in patients with asymptomatic hematuria. World J Urol. 2021;39(1):97-103. doi:10.1007/s00345-020-03171-6.Wolfman DJ, Marko J, Nikolaidis P, et al. ACR Appropriateness Criteria® hematuria. J Am Coll Radiol. 2020;17(5 Suppl):S138-S147. doi:10.1016/j.jacr.2020.01.028.