

Superficial Thrombophlebitis: Diagnosis, Ultrasound Imaging, and Management in Primary Care
Superficial thrombophlebitis can be challenging to diagnose, as many conditions mimic it, including serious diagnoses such as deep vein thrombosis. In this post, we review key differentials for acute leg swelling, along with diagnostic imaging pearls and follow-up recommendations for superficial thrombophlebitis.
What Is Superficial Thrombophlebitis?
Superficial thrombophlebitis is a condition in which blood clots develop within superficial veins near the skin surface, most commonly in the legs or arms (1).
Risk Factors and Clinical Presentation
Common risk factors include varicose veins, pregnancy and up to 12 weeks postpartum, recent trauma, surgery or immobility, and malignancy (1).
Additional contributors include intravenous catheter use, age over 60 years, oral contraceptives or hormone therapy, inherited thrombophilias, obesity, infection, and inflammatory conditions such as lupus (1).
Patients typically present with localized swelling, warmth, tenderness, and erythema along the course of a superficial vein. A palpable cord is a classic finding for superficial thrombophlebitis.
Risk of DVT and Pulmonary Embolism
Superficial vein thrombosis is not always benign. Clots can extend into the deep venous system, leading to deep vein thrombosis and potentially pulmonary embolism.
At the time of diagnosis, approximately 25% of patients with superficial thrombophlebitis have concurrent deep vein thrombosis. Risk factors for progression include male sex, cancer, and prior history of DVT (1).
Approach to Acute Leg Swelling
Now let’s illustrate management of this common presentation with a case: A 55-year-old female presents with acute left leg swelling, localized pain, and erythema.
What is your approach?
A structured differential helps ensure that serious conditions are not missed. Consider must-not-miss diagnoses alongside more common conditions.
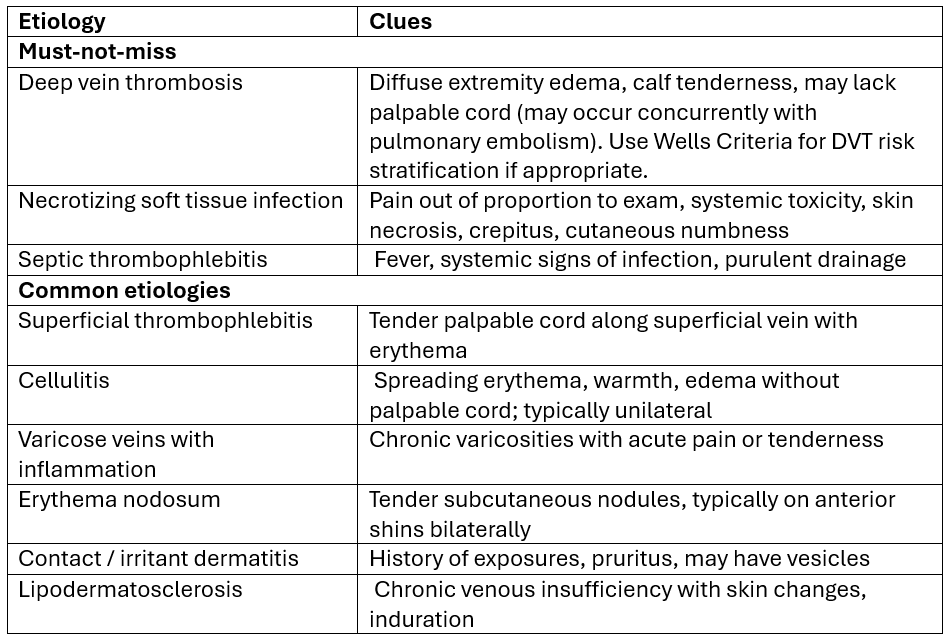
Source: 1,2 Note: list not exhaustive
Red Flags Requiring Urgent Evaluation
Some major red flags include:
Pain out of proportion to exam
Systemic toxicity
Skin necrosis or crepitus
New dyspnea or chest pain raises concern for pulmonary embolism
Diffuse limb swelling should prompt evaluation for deep vein thrombosis
Bottom line: Many of these conditions overlap clinically. History and physical examination alone may not be sufficient, which is why venous duplex ultrasound is often necessary to clarify the diagnosis (1).
Back to the case: The patient is hemodynamically stable with no red flags. On examination, there is a tender, palpable cord along a superficial vein with localized erythema and no diffuse swelling.
You suspect superficial thrombophlebitis. What is your next step?
Diagnostic Imaging: Venous Duplex Ultrasound for Suspected Superficial Thrombophlebitis
While superficial thrombophlebitis can be diagnosed clinically, compression ultrasound is recommended in most cases.
Ultrasound helps confirm the diagnosis, exclude concurrent deep vein thrombosis, and determine thrombus length and proximity to the saphenofemoral or saphenopopliteal junction. These details are critical for management decisions.
Ultrasound is particularly important when symptoms are above the knee, near the popliteal fossa, when DVT is suspected, or when patients have significant risk factors for venous thromboembolism (3).
Patients with small, localized thrombosis confined to varicose veins and no additional risk factors may not require imaging, though it is still commonly performed.
Bottom line: Duplex ultrasonography remains the reference standard for diagnosis and assessment of thrombus extent for suspected superficial thrombophlebitis cases.
Interpreting Imaging Findings & Management of Superficial Thrombophlebitis
Management depends on thrombus location, size, and proximity to the deep venous system.
When Anticoagulation Is Required
Patients with concurrent deep vein thrombosis should receive full therapeutic anticoagulation.
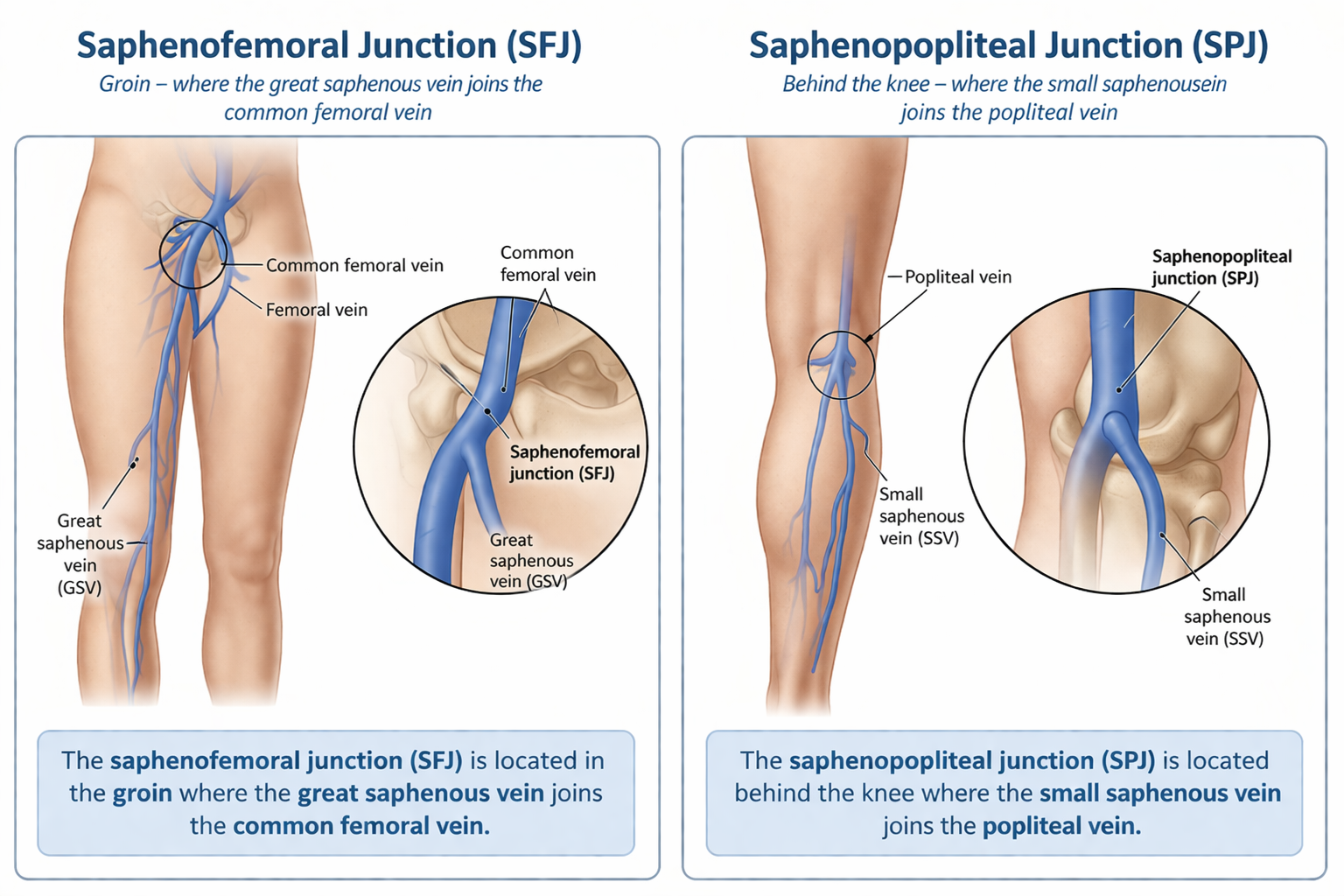
Isolated superficial thrombophlebitis within 3 cm of the saphenofemoral or saphenopopliteal junction carries a high risk of extension and should be treated with anticoagulation for approximately 3 months (2,3).
The saphenofemoral junction is located in the groin where the great saphenous vein joins the common femoral vein (4).
The saphenopopliteal junction (SPJ) is located behind the knee where the small saphenous vein joins the popliteal vein (4).
For isolated clots >5 cm in length and 3 cm from the deep system, prophylactic anticoagulation is recommended. Common options include fondaparinux 2.5 mg subcutaneously daily, rivaroxaban 10 mg orally daily, or low molecular weight heparin for 45 days (2,3).
Patients with shorter clots that are 3 cm from the deep system can be treated with oral or topical NSAIDs, compresses (warm or cool), and elevation for symptomatic relief. Compression stockings of appropriate length and tension can be considered if tolerable and no contraindications exist (e.g. known peripheral arterial disease) (3).
Patients with shorter clots >3 cm from the the deep system but significant symptoms or risk factors for extension (e.g. prior history or VTE, cancer, pregnancy, hormone therapy, recent surgery or trauma) may also be considered for prophylactic anticoagulation for up to 45 days (3).
For clots <5 cm or below the knee, repeat ultrasound in 7-10 days to assess for progression and determine the need for anticoagulation (2).
If not treating or if using topical NSAIDs only, monitor for extension with repeat ultrasound 7 to 10 days later. The goal of repeat ultrasound is to rule out extension into the deep veins, not to confirm resolution of thrombus which may take weeks or be present indefinitely (3).
When in doubt – consult hematology!
For specific treatment options - check our this table from Thrombosis Canada.
Bottom line: Superficial thrombophlebitis is common but not always benign. Always assess for extension into the deep system and tailor management based on clot size and location.
When Supportive Care Is Appropriate
For isolated superficial thrombophlebitis <5 cm in length and >3 cm from the deep venous system, supportive management is appropriate.
This includes oral or topical NSAIDs, warm or cool compresses, and limb elevation. Compression stockings may be used if tolerated and if there are no contraindications such as peripheral arterial disease (3).
Follow-up ultrasound in 7 to 10 days is recommended to assess for extension, particularly if anticoagulation is not initiated (2,3).
Bottom Line: Early identification of high-risk features with your clinical exam and ultrasound can prevent progression to deep vein thrombosis or pulmonary embolism.
Back to the case: Ultrasound confirms a superficial thrombus in the distal lower extremity, located more than 3 cm from the deep venous system and less than 5 cm in length.
You initiate conservative management with oral NSAIDs (e.g. ibuprofen 400 mg three times daily or naproxen 500 mg twice daily, assuming no contraindications). Supportive measures include warm or cold compresses and elevation.
You arrange follow-up in 7 to 10 days and provide return precautions, including worsening pain or swelling, spreading erythema, or new shortness of breath or chest pain.
💡For weekly diagnostic imaging insights and practice-changing pearls, join NP Reasoning Masterclass.
References
Angulo MI, Mauro AC, Vela M. What Is Superficial Vein Thrombosis? JAMA. 2026;335(6):560. doi:10.1001/jama.2025.20529Piazza G, Krishnathasan D, Hamade N, et al. Superficial Vein Thrombosis: A Review. JAMA. 2025;334(22):2020–2030. doi:10.1001/jama.2025.15222Thrombosis Canada. Superficial Thrombophlebitis. 2023. Available from https://thrombosiscanada.ca/clinical_guides/pdfs/90_26.pdfGloviczki P, Comerota AJ, Dalsing MC, et al. The care of patients with varicose veins and associated chronic venous diseases: clinical practice guidelines of the Society for Vascular Surgery and the American Venous Forum. J Vasc Surg. 2011;53(5 Suppl):2S-48S.Khan F, Tritschler T, Kahn SR, Rodger MA. Venous thromboembolism. Lancet. 2021 Jul 3;398(10294):64-77. doi: 10.1016/S0140-6736(20)32658-1. Epub 2021 May 10. PMID: 33984268.