

PCOS Differentials and Lab Test Interpretation
Amenorrhea or oligomenorrhea is a common primary care presentation. We’ll run through a practical framework from differentials, tailored testing, and how to confidently diagnose PCOS (without over-testing).
🔎Case: a 30-year-old female comes in to see you concerned about irregular periods. She hasn’t had one in about 2 months, and this is pretty typical for her. What is your approach to irregular periods (oligomenorrhea)?
First, let’s clarify a few terms:
Amenorrhea: the absence of menses (primary, or secondary – menses ceases for >3 months)
Oligomenorrhea: menstrual cycles occurring >35 days apart, generally having <6-8 periods/year
Next, I like to think of key differentials for Amenorrhea/Oligomenorrhea to help inform my history and physical exam:
Differentials for Amenorrhea/Oligomenorrhea
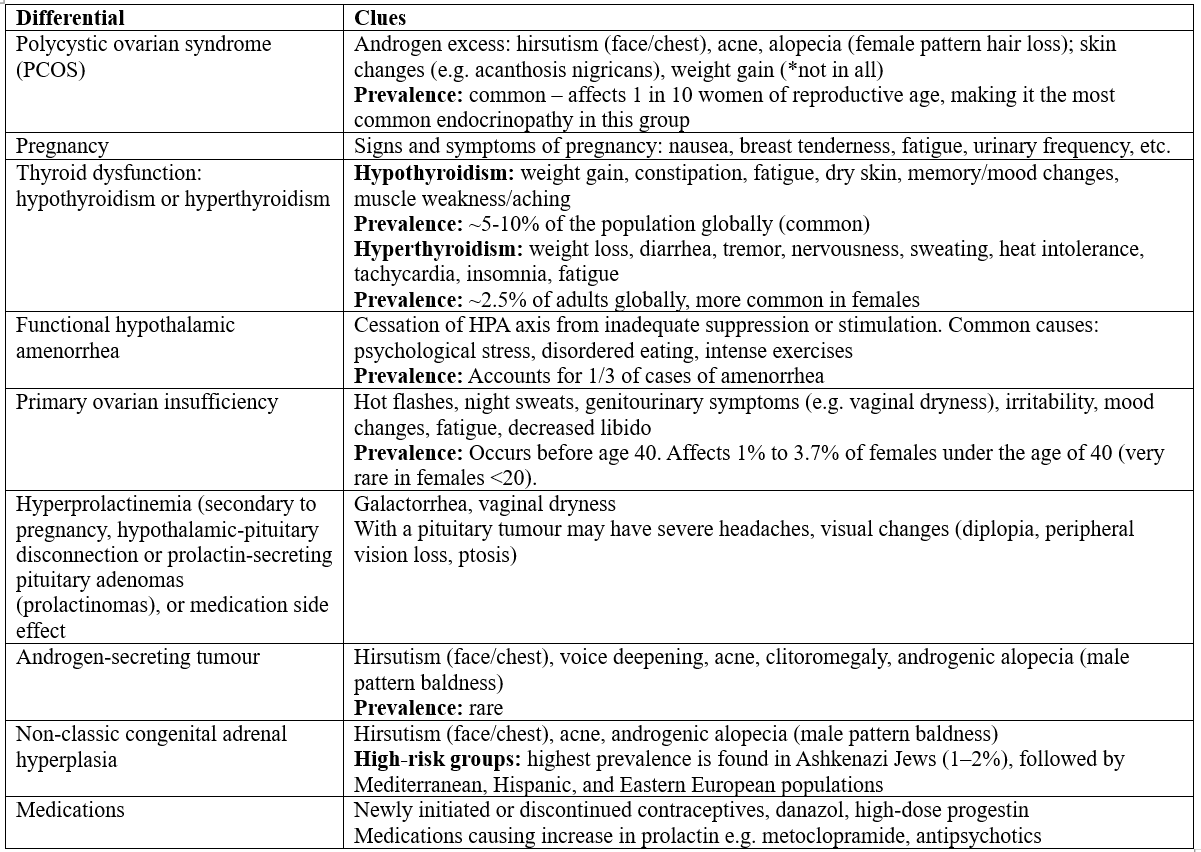
sources: 1,2
High-Yield History Questions
Duration: ask about history of irregular menses, pattern of menstrual cycles
Assess for pregnancy: sexually active, unprotected sex, use of birth control; symptoms such as nausea, vomiting, breast tenderness, fatigue, urinary frequency
Has there been any stress, diet, or exercise habits (history of eating disorder) that could affect menstrual cycles?
Screen for hyperandrogenism: hirsutism (face, chest, thighs, back), acne, alopecia, voice deepening, clitoromegaly
Screen for hyperprolactinemia: galactorrhea, vaginal dryness, severe headaches, vision changes
Screen for thyroid dysfunction: fatigue, dry skin, constipation or diarrhea, weight loss or weight gain, heat intolerance etc.
Age <40: screen for hot flashes, night sweats, vaginal dryness, mood changes, poor sleep, decreased libido
Medications: contraceptives and other hormone-containing drugs, medications causing increase in prolactin (e.g. metoclopramide, antipsychotics) (3)
Physical Exam Pearls
Height, weight, BMI: A BMI > 30 kg/m2 is observed in >50% of women with PCOS, depending on the population studied. Women with a BMI <18.5 kg/m2 may have functional hypothalamic amenorrhea due to an eating disorder, strenuous exercise, or a systemic illness associated with weight loss
Signs of hyperandrogenism: hirsutism, acne, alopecia (female pattern hair loss vs male pattern baldness)
Female pattern hair loss: diffuse, overall thinning on the top of the scale with a widening part (front hairline is often preserved)
Male pattern baldness: receding hairline and crown/vertex balding
Signs of hypothyroidism: e.g. bradycardia, dry skin
Signs of hyperthyroidism: e.g. tachycardia, diaphoresis, tremor (3)
🔎Back to the Case: she reports menstrual cycles ~40-45 days for the last 5 years. She has tried combining oral contraceptive medication in the past to help regulate her periods, and to help with facial and back acne, which helped but side effects made her discontinue them. She is not in a high-risk group for classic non-congenital adrenal hyperplasia.
She denies hot flashes, night sweats, genitourinary symptoms, galactorrhea or neurologic symptoms. She denies any changes to diet or exercise. She reports moderate fatigue. She is sexually active and uses condoms with her husband. She does not take any medication. She does plan on conceiving in the next few years.
On exam: BMI 30, stable vitals, mild-moderate facial and back acne, acanthosis nigricans suspected at the base of her neck. There is no voice deepening, alopecia, or hirsutism.
What differentials are we considering at this point?
Top of mind would include PCOS, rule out pregnancy, thyroid dysfunction, and hyperprolactinemia.
Less likely: primary ovarian insufficiency, prolactinoma, hyperandrogenism secondary to non-classic congenital adrenal hyperplasia, or an androgen-secreting tumour
What comes next?
The Rotterdam Criteria for PCOS
At this point, she meets the Rotterdam Criteria for PCOS (recap):
Required Features (2 of 3):
Ovulatory Dysfunction: Oligomenorrhea (periods >35 days apart) or amenorrhea (<8 cycles/year) ✅
Hyperandrogenism: Clinical (hirsutism, acne, alopecia) or biochemical (high free androgen index or total testosterone) ✅
Polycystic Ovaries (PCOM): Ultrasound shows 12 or more follicles (2–9 mm diameter) in at least one ovary or an ovarian volume (1,2)
Our pre-test probability for PCOS would be high at this point, but a standard work-up still includes ruling out common differentials (but we don’t need to go chasing everything if the history and physical exam are reassuring).
💡Bottom line: PCOS can be a clinical diagnosis. if a patient presents with oligomenorrhea and clinical signs of hyperandrogenism (hirsutism, acne, alopecia) and other common causes are ruled out, this is sufficient to diagnose PCOS.
Lab Tests for Amenorrhea/Oligomenorrhea
Rule out the more common etiologies first, tailor further tests based on your pre-test probability of disease from your history and physical exam.
Step #1
b-HCG: rule out pregnancy! Pregnancy is one of the most common causes of absent/irregular periods
Pearl: sensitivity and specificity of a qualitative (dip stick) bHCG exceeds 99% (no need to order a quantitative bHCG if you have a point of care test in office)
TSH: rule out thyroid disease
Prolactin: rule out hyperprolactinemia (assesses HPO axis status)
FSH: captures functional hypothalamic amenorrhea and other common causes (assesses HPO axis status)
Step #2
If there are signs of hyperandrogenism (hirsutism, acne, male-pattern baldness) – check a total testosterone (between 7:00 AM and 10:00 AM)
Pearl: don’t bother with a free testosterone, assays are not reliable
If they are a high-risk population for non-classic congenital adrenal hyperplasia – check a morning 17-OHP to check for late onset disease (very rare)
NOT recommended for initial testing:
DHEAS: this is an adrenal androgen looking for a much rarer cause (e.g. adrenal secreting tumour)
LH: provides similar information to FSH
Estradiol: is secreted by the ovaries by mature follicles and then the developing corpus luteum after ovulation. It will always be low in someone with secondary amenorrhea unless they have cervical obstruction that is preventing menses. Estradiol may also be normal in PCOS but is not diagnostic. If you suspect primary ovarian insufficiency, it is reasonable to order.
Anti-mullerian hormone (AMH): is an infertility test that reflects a patient's ovarian reserve. The level declines across the reproductive lifespan
(4,5)
Lab Interpretation Tips for PCOS and Beyond
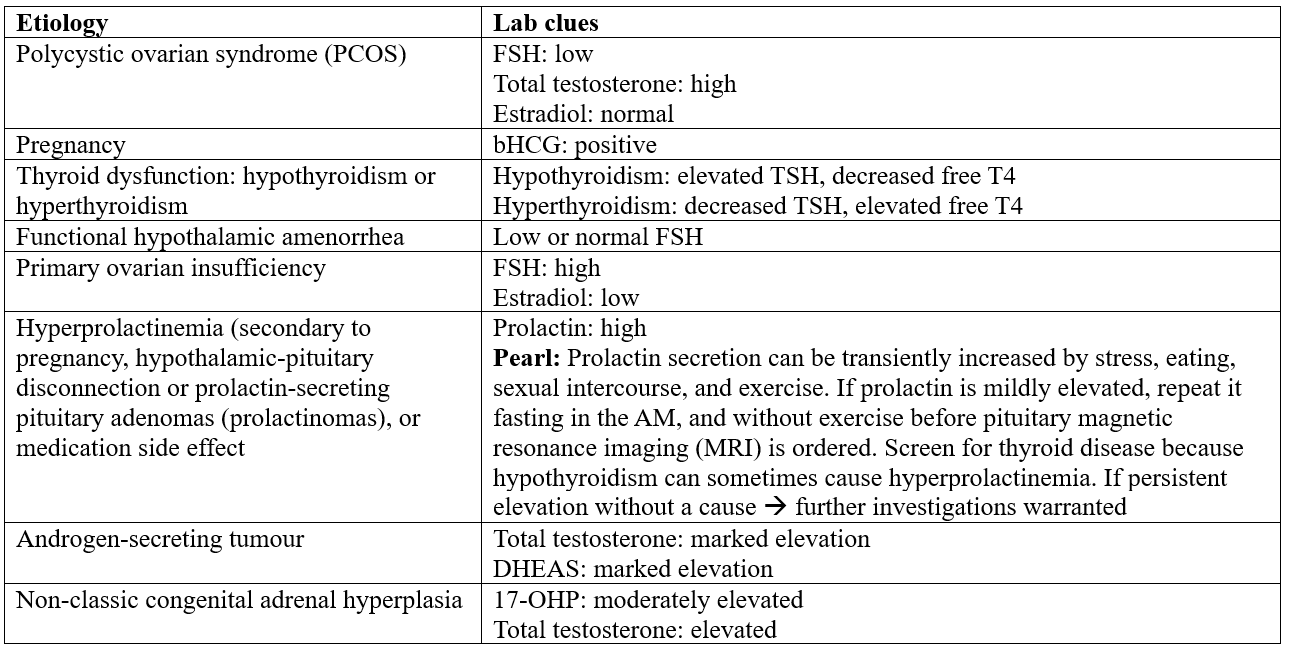
Sources: 4,5
💡Bottom line: Initial labs for amenorrhea/oligomenorrhea should include a bHCG, prolactin, TSH, FSH + total testosterone (if signs of hyperandrogenism) + 17-OHP (if from a high-risk group)
🔎Back to the case:
The following labs are ordered and results reviewed:
Qualitative bHCG: negative
TSH: normal
Prolactin: normal
FSH: low
Total testosterone (due to hyperandrogenism - acne): high
Diagnosis: PCOS based on the low FSH, high testosterone and normal TSH/prolactin. Pregnancy is also ruled out.
💡Practice Point: Nearly half of PCOS patients see 3+ providers before receiving a diagnosis – this is a common condition that warrants a high index of suspicion for any female of child baring age with irregular menses.
Diagnostic Imaging for PCOS
Do we need to order a pelvic ultrasound to diagnose PCOS?
Bottom line: PCOS can be diagnosed clinically, with oligomenorrhea and clinical signs of hyperandrogenism (or elevated total testosterone). If you still suspect PCOS and there is an absence of clinical signs and normal labs, a pelvic ultrasound can be arranged to look for polycystic ovarian morphology.
Ultrasound findings diagnostic of PCOS
Follicle number and size, not cysts, are relevant to an ultrasound diagnosis. The Rotterdam criteria (high sensitivity and specificity) includes:
The presence of 12 or more follicles in either ovary measuring 2 to 9 mm in diameter and/or
increased ovarian volume: >10 mL
One ovary fitting this definition is sufficient to define PCOM (6).
Transvaginal ultrasound has higher sensitivity and specificity compared to transabdominal ultrasound (but not all patients will feel comfortable with TVUS, so discuss this with your patient) (6).
For this patient, an ultrasound would not be necessary for the diagnosis of PCOS.
💡For weekly diagnostic imaging insights and practice-changing pearls, join NP Reasoning Masterclass.
ReferencesTeede HJ, Tay CT, Laven JJE, Dokras A, Moran LJ, Piltonen TT, et al. Recommendations from the 2023 international evidence-based guideline for the assessment and management of polycystic ovary syndrome. J Clin Endocrinol Metab. 2023;108(10):2447-2469. doi:10.1210/clinem/dgad463.Williams T, Moore JB, Regehr J. Polycystic ovary syndrome: common questions and answers. Am Fam Physician. 2023;107(3):264-272.Welt CK, Barbieri RL. Evaluation and management of secondary amenorrhea. In: Geffner ME, editor. UpToDate [Internet]. Waltham (MA): UpToDate; 2026 [cited 2026 Feb 26]. Available from: https://www.uptodate.com/contents/evaluation-and-management-of-secondary-amenorrheaGordon CM, Ackerman KE, Berga SL, Kaplan JR, Mastorakos G, Misra M, et al. Functional hypothalamic amenorrhea: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2017;102(5):1413-1439. doi:10.1210/jc.2017-00131.Klein DA, Paradise SL, Reeder RM. Amenorrhea: a systematic approach to diagnosis and management. Am Fam Physician. 2019;100(1):39-48.Barbieri RL, Ehrmann DA. Diagnosis of polycystic ovary syndrome in adults. In: Welt CK, editor. UpToDate [Internet]. Waltham (MA): UpToDate; 2026 [cited 2026 Feb 26]. Available from: https://www.uptodate.com/contents/diagnosis-of-polycystic-ovary-syndrome-in-adults