

Incidentaloma: Gallbladder Polyps
Case: an abdominal ultrasound was ordered for a patient with suspected metabolic-associated fatty liver disease.
Results: no calculi, few polyps identified, largest is pedunculated with thin stalk, and measures 4mm. Common bile duct: unremarkable. LIVER: unremarkable.
What is a gallbladder polyp? Gallbladder polyps are often discovered by accident—showing up in about 10% of upper abdominal ultrasounds. Most of the time, unless they are large, these polyps don’t cause symptoms (1). On ultrasound, a polyp looks like a small bump on the gallbladder wall that sticks into the lumen (the hollow inside). Unlike gallstones, polyps don’t move and don’t cast a shadow behind them on imaging (2,3).
Polyps → fixed to the gallbladder wall, may be stalk-like (pedunculated) or flat (sessile).
Gallstones → usually mobile and create a shadow on ultrasound
Differential Diagnosis for a Gallbladder Polyp
I like to think of 3 diagnostic buckets: benign, non-invasive neoplastic, and malignant. It is also important to differentiate gallstones from gallbladder polyps.
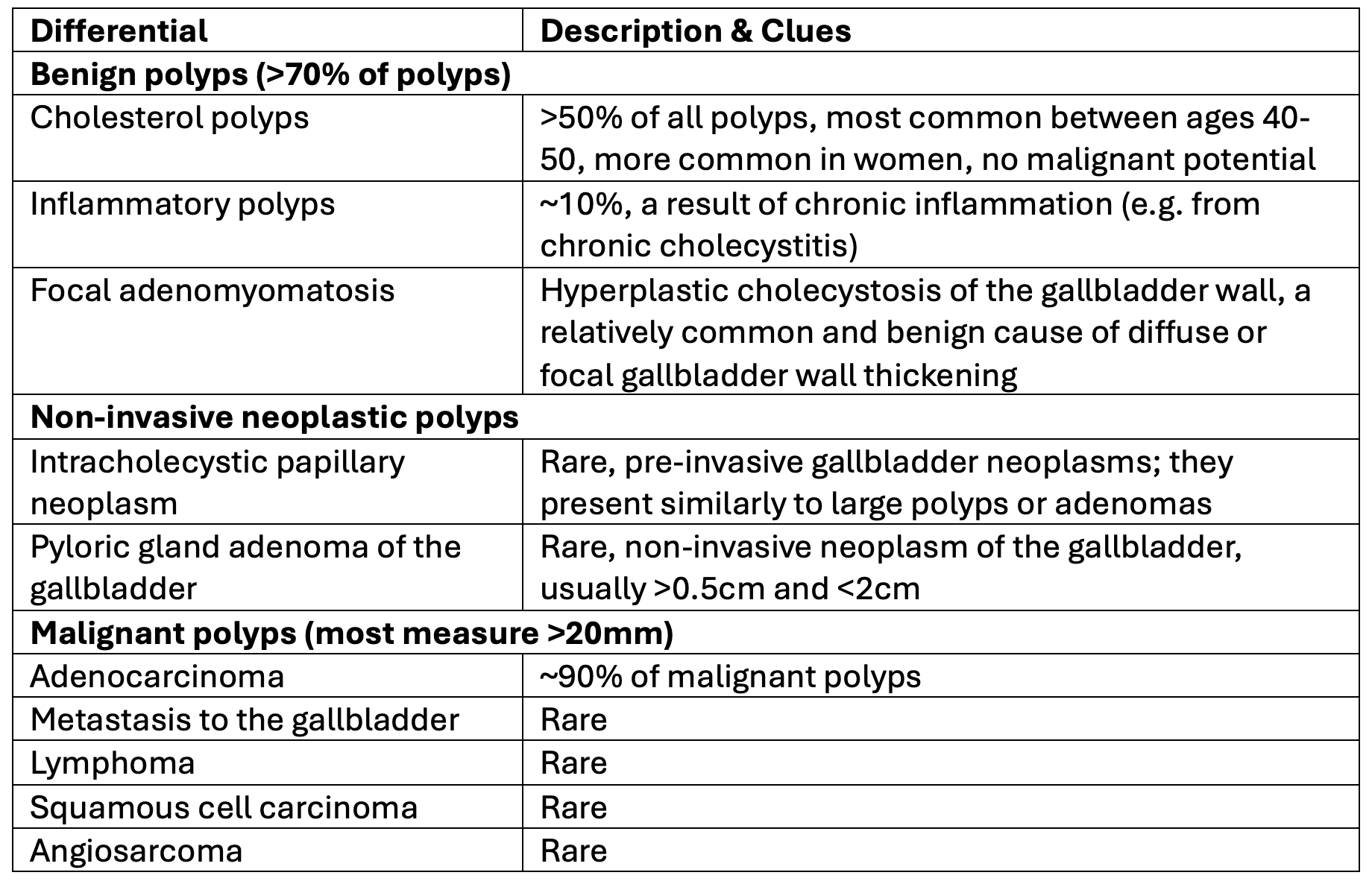
List not exhaustive. Source: 1
BOTTOM LINE: for a gallbladder polyp differential, we can think of benign, non-invasive neoplastic, and malignant polyps.
Radiographic Features of Gallbladder Polyps: Benign vs. Malignant
Think of size, morphology (shape), number, & growth to differentiate benign from malignant (1,4):
Size:
Benign: if <5mm, almost always cholesterol polyps.
Malignant: if >10mm, between 5-10mm warrant tracking growth.
Number:
Benign: >50% of cholesterol polyps are multiple.
Malignant: solitary lesion.
Growth:
Benign: no growth or stable growth
Malignant: growth over time
Other US features:
Benign: small echogenic focus or cluster of foci, comet tail artifact (cholesterol polyp)
Malignant: sessile polyp including focal gallbladder wall thickening <4mm (2)
BOTTOM LINE: malignant features on ultrasound include size >10mm, solitary lesion, growth over time, and sessile morphology with focal gallbladder wall thickening.
History Clues
Always take pre-test probability into account, in addition to ultrasound findings. The following history clues may increase your pre-test probability of a malignant polyp:
A history of primary sclerosing cholangitis (2,4)
Age >50 (3)
Ethnicity: south asian
Back to the case: The patient is a 40-year-old Caucasian female. There is no history of primary sclerosing cholangitis, and they are currently asymptomatic.
Gallbladder Polyp: Follow-up and Management
Let’s review a few guidelines to compare management:
Canadian Association of Radiologists (CAR) + Society of Radiologists in Ultrasound (SRU) (2022)
The CAR Incidental Findings Working Group has released an update to its 2020 recommendations for managing gallbladder polyps found by chance on imaging. This revision was driven by new research and recently published international guidelines.
In reviewing the evidence, the group compared the 2022 Society of Radiologists in Ultrasound (SRU) Consensus Statement with the 2022 joint European guidelines. The new CAR update leans toward the SRU’s risk-based approach, which focuses on polyp characteristics such as morphology. This marks a move away from routine follow-up and intervention for small, low-risk polyps, and toward a more tailored strategy (5). Gallbladder polyps are risk-stratefied as:
Extremely low risk: pedunculated, ball-on-the-wall or pedunculated with thin stalk (6).
<9mm: no follow up
10-14mm: follow up US at 6, 12, 24 months
>15mm: surgical consult
Low risk: Pedunculated with thick or wide stalk, or sessile (6).
<6mm: no follow up
7-9mm: follow up US at 12 months
10-14mm: follow up US at 6, 12, 24, 26 months vs surgical consult
>15mm: surgical consult
Intermediate risk: focal wall thickening >4mm adjacent to polyp (6)
<6mm: follow up US at 6, 12, 24, 36 months vs surgical consult
>7mm: surgical consult
On follow up:
If increase of >4mm in <12 months OR reaches threshold within category - recommend surgical consult (6)
Decrease of >4mm - stop following
American College of Radiology Guidelines (2013)
Proposes a size-based criteria for follow up and management (7):
<6mm: no follow up
7-9mm: annual US to ensure no growth; surgical consult if polyp grows. If a patient is at higher risk (>50, sessile or single polyp, Asian ethnicity, follow up US at 6 months, then yearly)
>10mm: surgical consultation for cholecystectomy
European Guidelines (2021)
These joint guidelines consider size and individual patient risk factors to guide follow up and management — see the algorithm here (8).
Start with size:
>10mm: surgical consult recommended
<10mm: are they symptomatic or asymptomatic?
Symptomatic: Symptoms attributed to gallbladder disease: surgical consult recommended
Asymptomatic: ask - do they have risk factors for malignancy? (age >60, primary sclerosing cholangitis, Asian ethnicity, sessile polyp with focal wall thickening >4mm)
YES risk factors for malignancy are present:
Polyp <5mm: US (6 - 12 - 24 months)
Polyp 6-9 mm: surgical consult
NO risk factors for malignancy:
Polyp <5mm: no f/u
Polyp 6-9 mm: US (6 – 12 – 24 months)
If a patient has a solitary polyp PLUS a risk factor for malignancy, this increases the pre-test probability for a malignant lesion and surgical referral should be considered (8).
With serial imaging, if the polyp reaches 10mm, surgical consult is recommended (8).
If the polyp grows by 2mm or more within the 2 year follow up, it’s current size should be reviewed along with risk factors and symptoms, consider a surgical consult (8).
If the polyp disappears, discontinue imaging follow-up (8).
BOTTOM LINE: there are several guidelines to help determine management of gallbladder polyps.
Back to the case:
Results review the US findings again: no calculi, few polyps identified, largest is pedunculated with think stalk and measures 4mm. Common bile duct: unremarkable. LIVER: unremarkable.
The patient is asymptomatic. No risk factors for malignancy.
Follow-up plan: using the CAR/SRU guidelines, no follow-up imaging is recommended, given the extremely low-risk features, absence of risk factors, and small size. As always, follow local guidelines.
Want curated education to make confident & informed decisions with your patients? 👉 Sign up for NP Reasoning Masterclass.
References Weerakkody Y, Di Muzio B, Knipe H, et al. Gallbladder polyp. Reference article, Radiopaedia.org (Accessed on 25 Aug 2025) https://doi.org/10.53347/rID-7604Wiles R, Thoeni RF, Barbu ST, Vashist YK, Rafaelsen SR, Dewhurst C, Arvanitakis M, Lahaye M, Soltes M, Perinel J, Roberts SA. Management and follow-up of gallbladder polyps : Joint guidelines between the European Society of Gastrointestinal and Abdominal Radiology (ESGAR), European Association for Endoscopic Surgery and other Interventional Techniques (EAES), International Society of Digestive Surgery - European Federation (EFISDS) and European Society of Gastrointestinal Endoscopy (ESGE). Eur Radiol. 2017 Sep;27(9):3856-3866. doi: 10.1007/s00330-017-4742-y. Epub 2017 Feb 9. PMID: 28185005; PMCID: PMC5544788.Jones MW, Deppen JG. Gallbladder Polyp. [Updated 2023 Aug 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470211/Gaillard F, Haouimi A, Morgan M, et al. Benign vs malignant features of gallbladder polyps. Reference article, Radiopaedia.org (Accessed on 25 Aug 2025) https://doi.org/10.53347/rID-9716Fung CI, Kamaya A, Brahm GL, Bird JR, Kirkpatrick IDC. Recommendations for the Management of Incidentally Detected Gallbladder Polyps: Update of the 2020 Canadian Association of Radiologists Recommendations for the Management of Incidental Hepatobiliary Findings in Adults. Canadian Association of Radiologists Journal. 2025;0(0). doi:10.1177/08465371251346728Kamaya A, Fung C, Szpakowski J, et al. Management of incidentally detected gallbladder polyps: society of radiologists in ultrasound consensus conference recommendations. Radiology. 2022;305(2):277-289.Sebastian S, Araujo C, Neitlich J, Berland L. Managing Incidental Findings on Abdominal and Pelvic CT and MRI, Part 4: White Paper of the ACR Incidental Findings Committee II on Gallbladder and Biliary Findings. J Am Coll Radiol. 2013;10(12):953-6. doi:10.1016/j.jacr.2013.05.022 - PubmedFoley KG, Lahaye MJ, Thoeni RF, Soltes M, Dewhurst C, Barbu ST, Vashist YK, Rafaelsen SR, Arvanitakis M, Perinel J, Wiles R, Roberts SA. Management and follow-up of gallbladder polyps: updated joint guidelines between the ESGAR, EAES, EFISDS and ESGE. Eur Radiol. 2022 May;32(5):3358-3368. doi: 10.1007/s00330-021-08384-w. Epub 2021 Dec 17. PMID: 34918177; PMCID: PMC9038818.